Correction of hand deformities after burns
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Institute for Medical Science, Keimyung University School of Medicine, Daegu, Korea
- KMID: 2526644
- DOI: http://doi.org/10.12790/ahm.21.0131
Abstract
- Hand burns can lead to deformities even after successful primary healing. They are the most common cause of skin contracture involving the hand. This review article discusses ways to correct claw deformity, flexion contracture in the palm and finger, and web space contracture, which are post-burn hand deformities commonly encountered in clinical practice. Loss of skin is the end result in many cases of hand deformities after burns. Therefore, reinforcing the lost skin is the principle of corrective surgery. Even if the skin is thicker than the full-thickness skin, it will engraft if damage to the tissue and blood vessels of the recipient is minimized. The thicker the skin, the less re-contraction and growth occur. The foot is an ideal donor site for skin grafts on the hand. In particular, the instep or the area below the malleolar is a very good donor site. The first web space of the hand is very important for hand function, and it must be reconstructed with Z-plasty, a skin graft, and a free flap step by step according to the degree of contraction.
Keyword
Figure
-

Fig. 1. Claw hand deformity after a hand burn. A deformation in which the metacarpophalangeal joint is excessively extended and the interphalangeal joint is flexed is shown.

Fig. 2. Tangential excision and full-thickness skin graft. If complete flexion of the metacarpophalangeal joint is difficult due to burn scar formation on the back of the hand, complete flexion can be achieved by removing all of the scar tissue, followed by full-thickness skin graft surgery.

Fig. 3. (A, B) A 10-month-old boy who suffered a steam burn from a pressure rice cooker and developed flexion contracture in the palm, long, ring, and little fingers after conservative management. (C, right) The scar tissue was completely removed and a full-thickness skin graft from the groin was performed to correct the flexion contracture. (C, left) Ten days after skin graft.
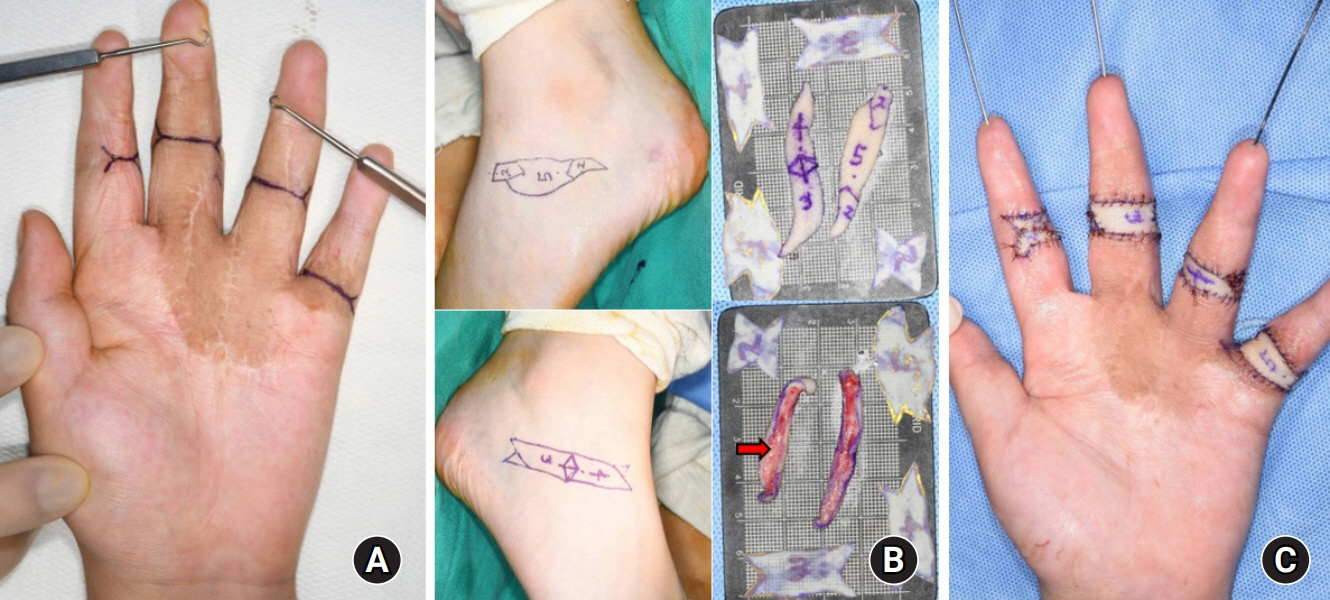
Fig. 4. (A) The flexion contracture recurred in the same boy as described in Fig. 3, at the age of 10 years. (B, C) After contracture release via a fish-mouth incision, a full-thickness skin with partial subcutaneous fat (red arrow) from both inferior malleolar areas was grafted and the fingers were immobilized with Kirschner wires.
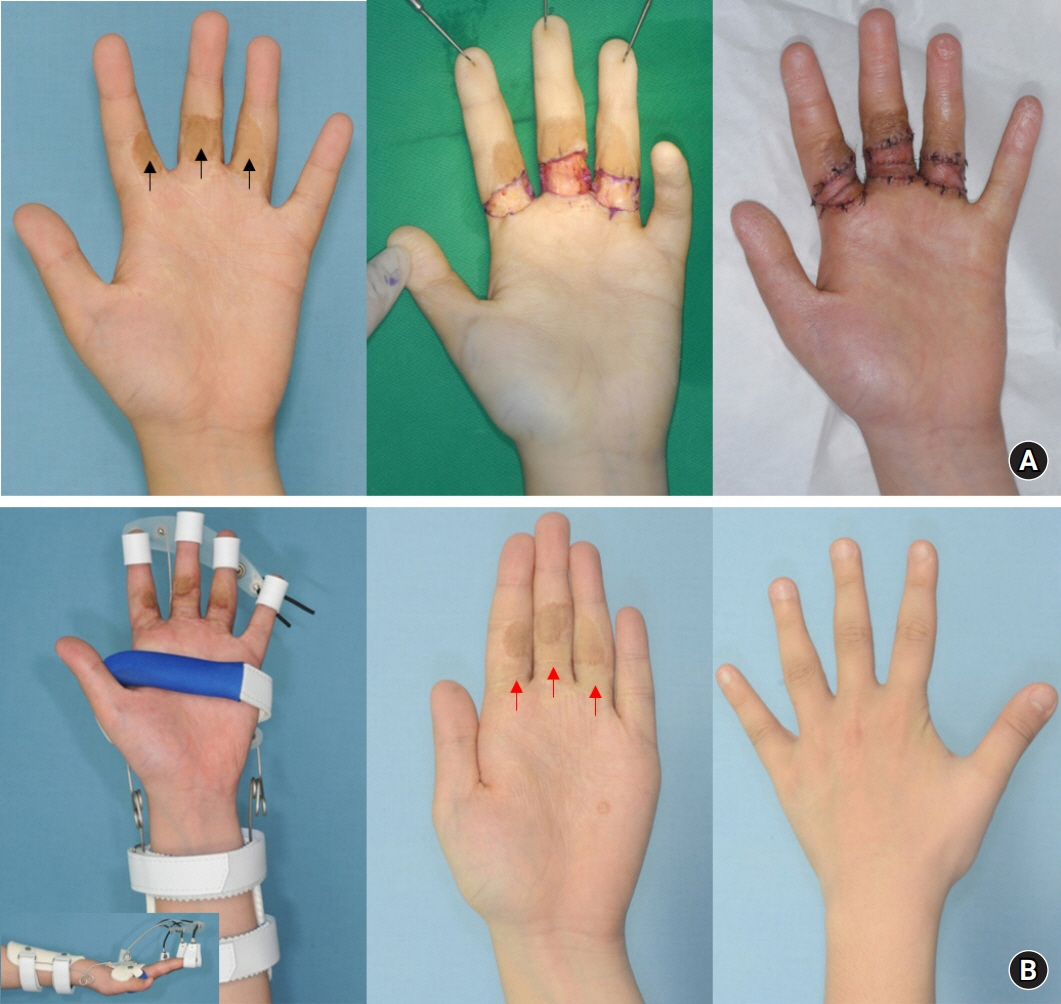
Fig. 5. (A, left) An 11-year-old boy, who sustained a burn at 1 year of age and was treated with a full-thickness skin graft from the groin, shows residual pigmentation (black arrows). (A, middle and right) On day 9 after the full-thickness skin graft with a part of subcutaneous fat from both inferior medial malleolar areas after complete release of the flexion contracture. (B, left) Wearing a dynamic splint. (B, middle) The color match of the grafted skin (red arrows) is excellent 3 years after surgery.
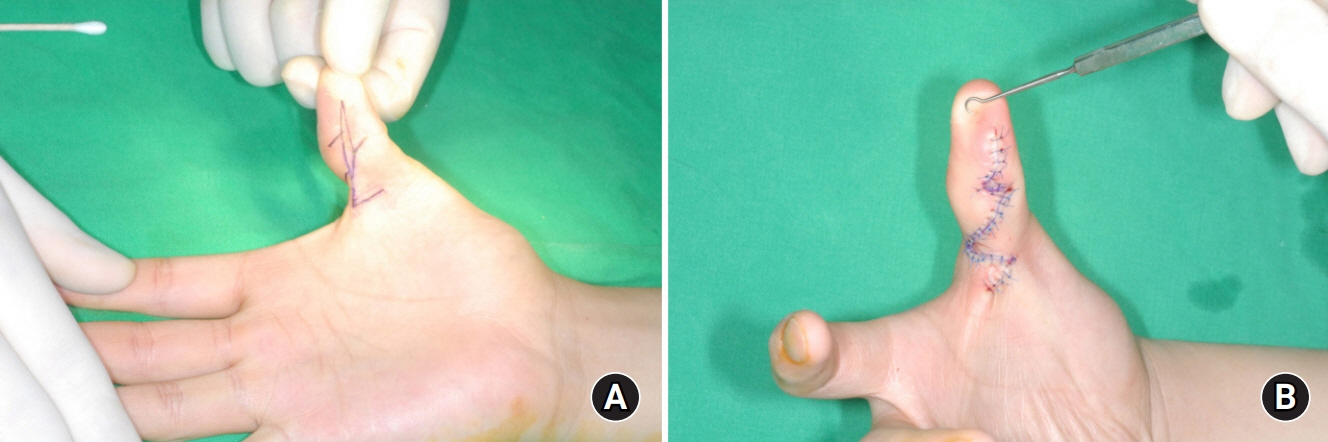
Fig. 6. (A) The flexion contracture caused by a narrow and long scar on the volar side of the thumb was corrected with multiple Z-plasty. (B) After flap transposition.
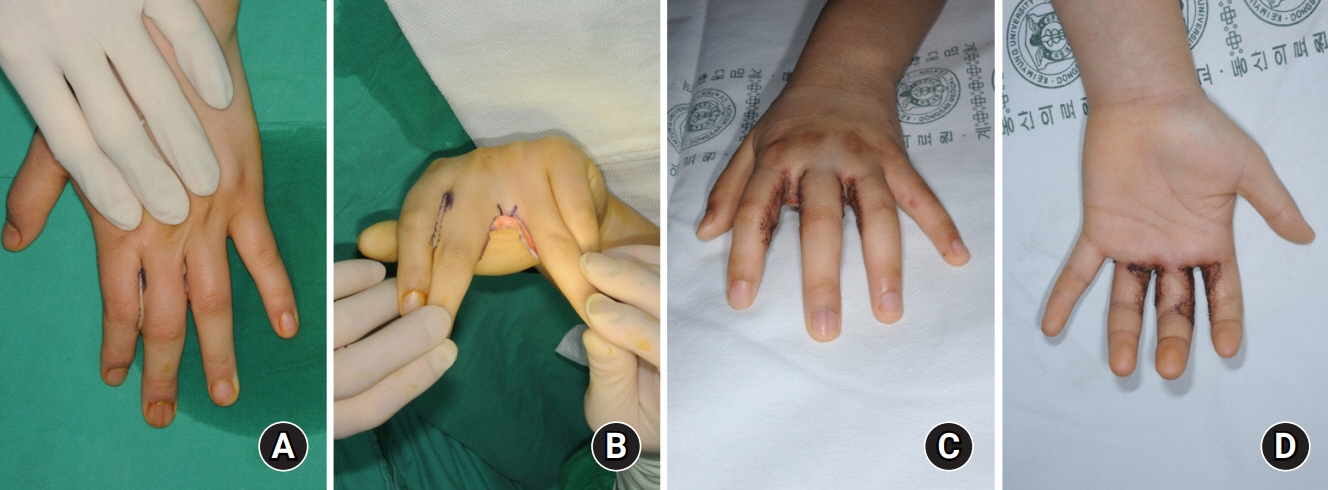
Fig. 7. (A) Syndactyly developed due to adhesion of the adjacent fingers after a burn. (B) Recurrence can be prevented by completely removing the scar tissue, securing enough interdigital web space with a releasing incision, (C, D) followed by grafting of sufficient full-thickness skin.

Fig. 8. (A) Syndactyly in a 6-year-old boy, who was exposed to a steam burn at 10 months of age. Syndactyly occurred as the web space moved distally due to flexion contracture of the fingers. The first operation on this patient was a skin graft for contracture at 7 months of age. (A, middle) During a second operation, flexion contracture and web space were released and a full-thickness skin graft was performed. (A, right) The photograph was taken 6 months after the operation, and the syndactyly was completely corrected. (B, left and middle) Syndactyly recurred at the age of 15 years, and the same operation was performed a third time. (B, right) At the age of 22 years, syndactyly recurred, and the fourth and final corrective surgeries were performed.

Fig. 9. (A) A contracting band and scar tissue in the first web space are noted. (B) Design of single large Z-plasty. (C) Complete excision of the contracting band and scar tissue before transferring the triangular flaps to each other. (D) After flap transposition.
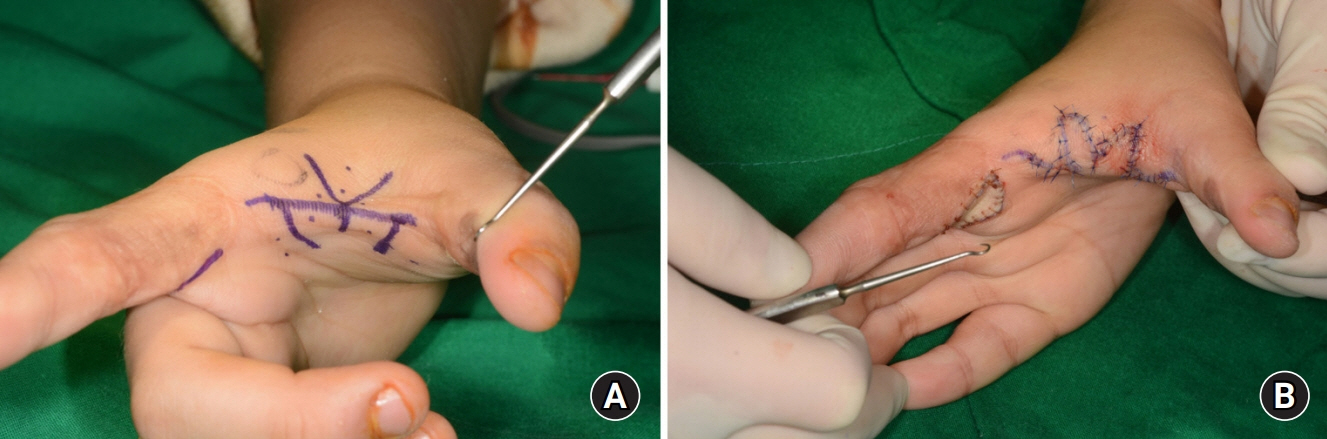
Fig. 10. (A) Design of double-opposing Z-plasty in the first web space. (B) After flap transposition.

Fig. 11. (A,B) In order to create the first and second web space, an incision was made on the contracture, followed by sufficient web space and a full-thickness skin graft. A Kirschner wire is very useful not only for immobilization and securing space, but also for engraftment of thick skin. (C) The web spaces were well maintained.
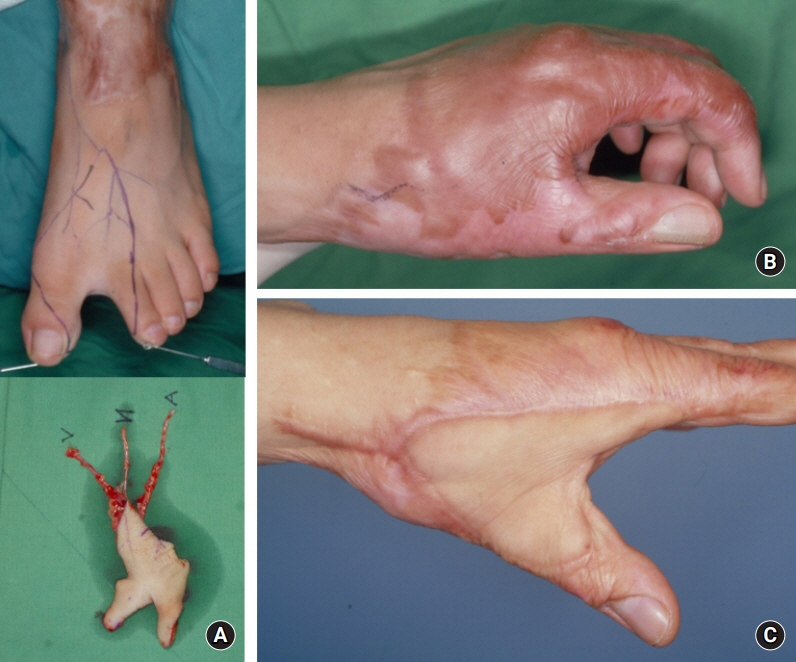
Fig. 12. (A) Design of a foot-first web space free flap is shown. (B) A hypertrophic scar is covered on the dorsum of the hand, including the first web space, which prevents full abduction of the thumb. (C) Appearance after reconstructive surgery.

Fig. 13. (A) A 23-year-old female patient had severe adduction contracture in the first web space after suffering a flame burn 18 months previously. (B) Release of the adductor and first dorsal interosseous muscles (red arrows) was followed by correction of adduction and supination of the metacarpal bone of the thumb and compensatory hyperextension of the metacarpophalangeal joint. (C) Reconstruction was followed by covering the defect with dorsalis pedis free flap.

Fig. 14. (A) The palm and first web space were damaged by the inlet of a high-voltage electric burn. (B) The toes were in contact with an electrical outlet. (C) The palm defect including the first web space was reconstructed with an anterolateral thigh free flap.
Reference
-
References
1. Whitson TC, Allen BD. Management of the burned hand. J Trauma. 1971; 11:606–14.
Article2. McKee DM. Acute management of burn injuries to the hand and upper extremity. J Hand Surg Am. 2010; 35:1542–4.
Article3. McCauley RL. Reconstruction of the pediatric burned hand. Hand Clin. 2000; 16:249–59.
Article4. Donalon MB. Reconstruction of the burned hand and upper extremity. In : May JW, Littler JW, editors. The hand. Philadelphia: W.B. Sanders;1990. p. 5452–82.5. Cauley RP, Helliwell LA, Donelan MB, Eberlin KR. Reconstruction of the adult and pediatric burned hand. Hand Clin. 2017; 33:333–45.
Article6. De la Garza M, Sauerbier M, Günter G, et al. Microsurgical reconstruction of the burned hand and upper extremity. Hand Clin. 2017; 33:347–61.
Article7. Kurtzman LC, Stern PJ. Upper extremity burn contractures. Hand Clin. 1990; 6:261–79.
Article8. Son D, Jeong H, Choi T, Kim J, Han K. A new mechanism associated with compositae graft success. J Plast Reconstr Aesthet Surg. 2010; 63:1900–9.
Article9. Son D, Jeong H, Choi T, Kim J, Han K. Preserved superficial fat skin composite graft for correction of burn scar contracture of hand. J Korean Soc Plast Reconstr Surg. 2008; 35:716–22.10. Won DC, Son DG, Han KH, Park KK. Accelerated healing of composite graft in a wet environment: a pig model. J Korean Soc Plast Reconstr Surg. 2003; 30:801–8.11. Son D, Han K, Chang DW. Extending the limits of fingertip composite grafting with moist-exposed dressing. Int Wound J. 2005; 2:315–21.
Article12. Son D, Park S, Kim H. Medial side of the foot as a skin graft donor site for correction of burn scar contracture of the hand. J Korean Soc Surg Hand. 2005; 10:136–41.13. Roh TS, Kim YS, Burm JS, Chung CH, Kim JB, Oh SJ. Rice cooker steam hand burn in the pediatric patient. Plast Reconstr Surg. 2000; 106:76–80.
Article14. Kreymerman PA, Andres LA, Lucas HD, Silverman AL, Smith AA. Reconstruction of the burned hand. Plast Reconstr Surg. 2011; 127:752–9.
Article15. Gulgonen A, Ozer K. The correction of postburn contractures of the second through fourth web spaces. J Hand Surg Am. 2007; 32:556–64.
Article16. Iwuagwu FC, Wilson D, Bailie F. The use of skin grafts in postburn contracture release: a 10-year review. Plast Reconstr Surg. 1999; 103:1198–204.
Article17. Greyson MA, Wilkens SC, Sood RF, Winograd JM, Eberlin KR, Donelan MB. Five essential principles for first web space reconstruction in the burned hand. Plast Reconstr Surg. 2020; 146:578e–587e.
Article18. Choi TH, Son DG, Han K. Classification and reconstructive strategies of first web space contracture. J Korean Soc Plast Reconstr Surg. 2001; 28:522–30.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis and Treatment of Postburn Hand Deformities Durn to Burn Scar Contracures in Children
- Optimizing Outcomes in the Reconstruction of Postburn Scar Hand Deformities
- The Management of Pediatric Steam Burn Caused by Electric Rice-cooker
- Clinical observation on pediatric hand burns
- Reconstruction of Severe Burn Scar Deformities on the Distal Nose and Philtrum
