A Gastrobronchial Fistula Secondary to Endoscopic Internal Drainage of a Post-Sleeve Gastrectomy Fluid Collection
- Affiliations
-
- 1Department of Gastroenterology, Hepatopancreatology and Digestive Oncology, Erasme University Hospital, Université Libre de Bruxelles, Brussels, Belgium
- KMID: 2525061
- DOI: http://doi.org/10.5946/ce.2021.033
Abstract
- A 44-year-old woman underwent sleeve gastrectomy, which was complicated by a leak. She was treated with two sessions of endoscopic internal drainage using plastic double-pigtail stents. Her clinical evolution was favorable, but four months after the initial stent placement, she became symptomatic, and a gastrobronchial fistula with the proximal end of the stents invading the diaphragm was diagnosed. She was treated with antibiotics, plastic stents were removed, and a partially covered metallic esophageal stent was placed. Eleven weeks later, the esophageal stent was removed with no evidence of fistula. Inappropriate stent size, position, stenting duration, and persistence of low-grade inflammation could explain the patient’s symptoms and provide a mechanism for gradual muscle rupture and fistula formation. Although endoscopic internal drainage is usually safe and effective for the management of post-laparoscopic sleeve gastrectomy leaks, close clinical and radiological follow-up is mandatory.
Keyword
Figure
-

Fig. 1. (A, B) Post-laparoscopic sleeve gastrectomy leak communicating with subphrenic fluid collection appeared opacified during gastroscopy. (C) Endoscopic internal drainage was performed by deployment of two double-pigtail stents with the proximal part in the collection and the distal part in the gastric sleeve. (D) Initial stents were removed endoscopically two months later. (E) Contrast injection showed persistence of collection but no sign of fistula. (F) Deployment of three new stents was done.

Fig. 2. (A) Computed tomography demonstrated double-pigtail stents invading the diaphragm. (B, C) Inflammatory collection with presence of a hydroaeric level around the stents and opacification of the left lower bronchus communicating with them was seen.
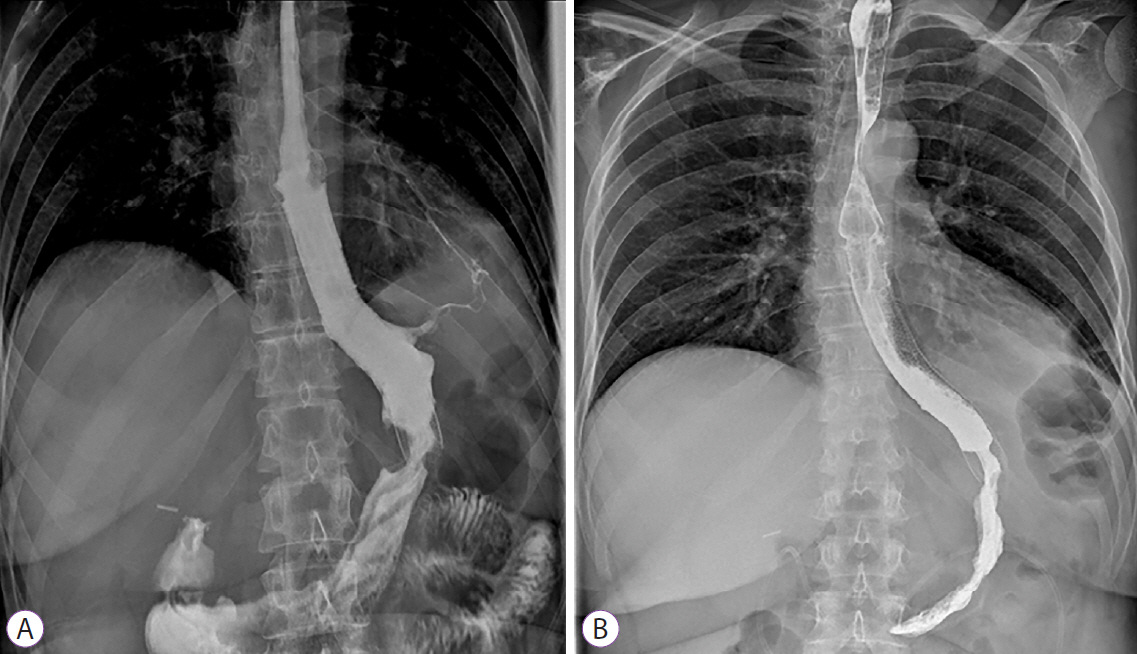
Fig. 3. (A) A gastrobronchial fistula was demonstrated during barium swallow study four days after esophageal stent deployment. (B) Three weeks later, esophagogram showed sealing of the two ends of the esophageal stent with distal and proximal hyperplasia and no sign of fistula persistence was evident.
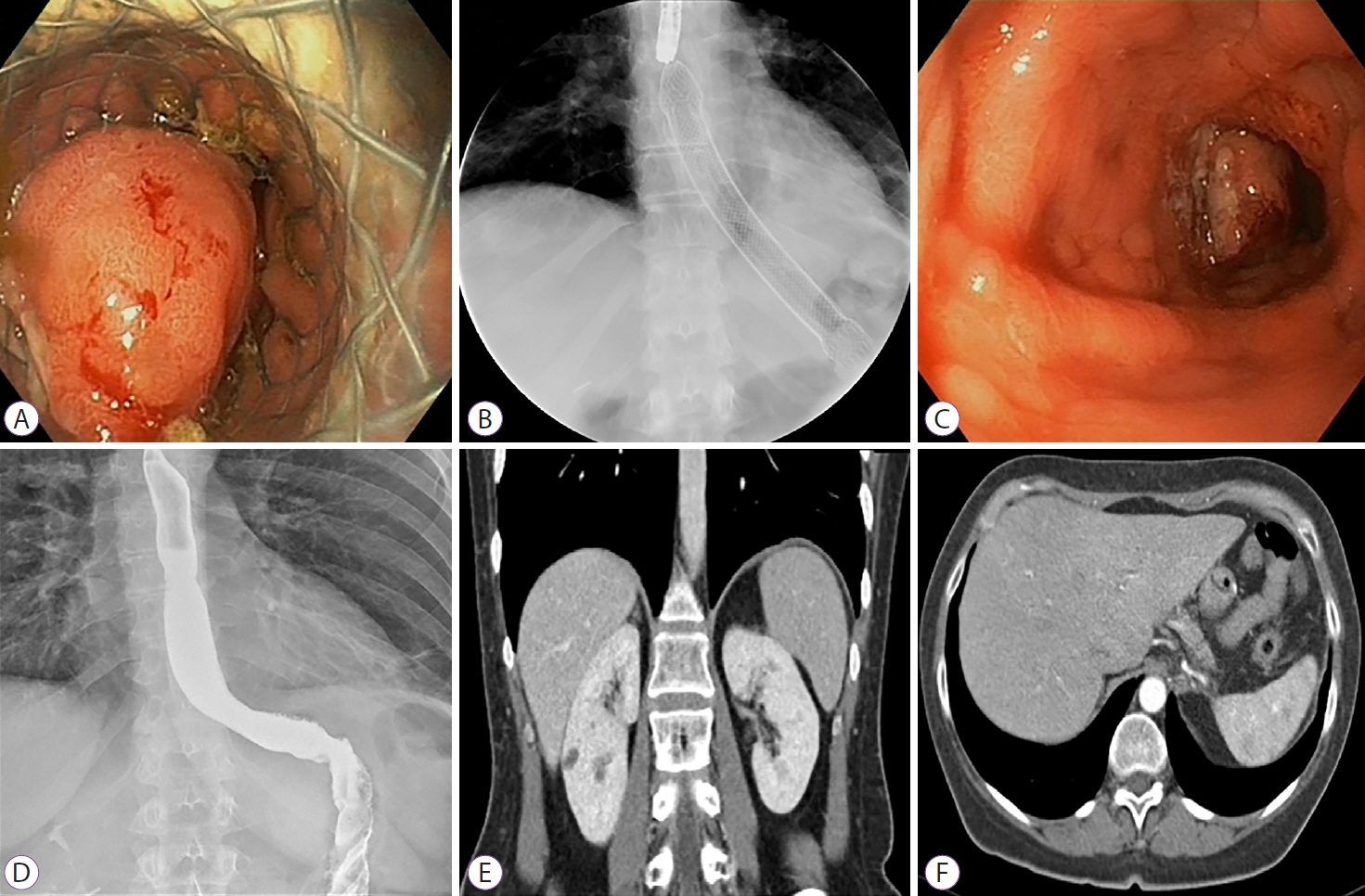
Fig. 4. (A, B, C) A second fully-covered metallic stent was used to remove the initial partially covered esophageal stent (stent-in-stent technique). (D, E, F) Follow-up esophagogram and computed tomography showed no evidence of residual fistula.
Reference
-
1. Eisendrath P, Deviere J. Major complications of bariatric surgery: endoscopy as first-line treatment. Nat Rev Gastroenterol Hepatol. 2015; 12:701–710.2. Donatelli G, Dumont JL, Cereatti F, et al. Endoscopic internal drainage as first-line treatment for fistula following gastrointestinal surgery: a case series. Endosc Int Open. 2016; 4:E647–E651.3. Gonzalez JM, Lorenzo D, Guilbaud T, Bege T, Barthet M. Internal endoscopic drainage as first line or second line treatment in case of postsleeve gastrectomy fistulas. Endosc Int Open. 2018; 6:E745–E750.4. Silva LB, Moon RC, Teixeira AF, et al. Gastrobronchial fistula in sleeve gastrectomy and roux-en-y gastric bypass--a systematic review. Obes Surg. 2015; 25:1959–1965.5. Siddique I, Alazmi W, Al-Sabah S. Endoscopic internal drainage by double pigtail stents in the management of laparoscopic sleeve gastrectomy leaks. Surg Obes Relat Dis. 2020; 16:831–838.6. Donatelli G, Ferretti S, Vergeau BM, et al. Endoscopic internal drainage with enteral nutrition (EDEN) for treatment of leaks following sleeve gastrectomy. Obes Surg. 2014; 24:1400–1407.7. Donatelli G, Catheline JM, Dumont JL, et al. Outcome of leaks after sleeve gastrectomy based on a new algorithm addressing leak size and gastric stenosis. Obes Surg. 2015; 25:1258–1260.8. Bouchard S, Eisendrath P, Toussaint E, et al. Trans-fistulary endoscopic drainage for post-bariatric abdominal collections communicating with the upper gastrointestinal tract. Endoscopy. 2016; 48:809–816.9. Lorenzo D, Guilbaud T, Gonzalez JM, et al. Endoscopic treatment of fistulas after sleeve gastrectomy: a comparison of internal drainage versus closure. Gastrointest Endosc. 2018; 87:429–437.10. Donatelli G, Airinei G, Poupardin E, et al. Double-pigtail stent migration invading the spleen: rare potentially fatal complication of endoscopic internal drainage for sleeve gastrectomy leak. Endoscopy. 2016; 48(Suppl 1 UCTN):E74–E75.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Case Report: Gastrobronchial Fistula after Sleeve Gastrectomy: Treated by Laparoscopic Proximal Gastrectomy with Double Tract Reconstruction
- Recurrent Gastrobronchial Fistula after Esophagectomy: one case report
- The Causes, Prevention, and Management of Gastric Leakage after Laparoscopic Sleeve Gastrectomy: A Review Article
- Endoscopic Management of Staple Line Leak after Bariatric Surgery: Surgeon’s Perspective
- A Case of Endoscopic Closure to Postoperative Leak after Laparoscopic Sleeve Gastrectomy in Patient with Morbid Obesity
