Importance of Differential Diagnosis of a Possible Brain Tumor in Patients with Cervical Radiculopathy
- Affiliations
-
- 1Department of Neurosurgery, Dankook University Hospital, Cheonan, Korea
- KMID: 2523923
- DOI: http://doi.org/10.3340/jkns.2021.0127
Abstract
- Lesions occurring simultaneously in the somatosensory or motor cortex of the brain and the cervical spine are rare. Brain tumors can cause similar symptoms to cervical lesions which can lead to confusion in treatment priorities. Moreover, if cervical disease is noticeably observed in radiologic findings of a patient complaining of cervical radiculopathy with non-specific electromyography results, it is common to no longer perform further evaluation. Here we introduce two cases where the cause of cervical radiculopathy was first considered to be the result of a degenerative cervical disease but was later discovered to be a result of a brain tumor.
Keyword
Figure
-
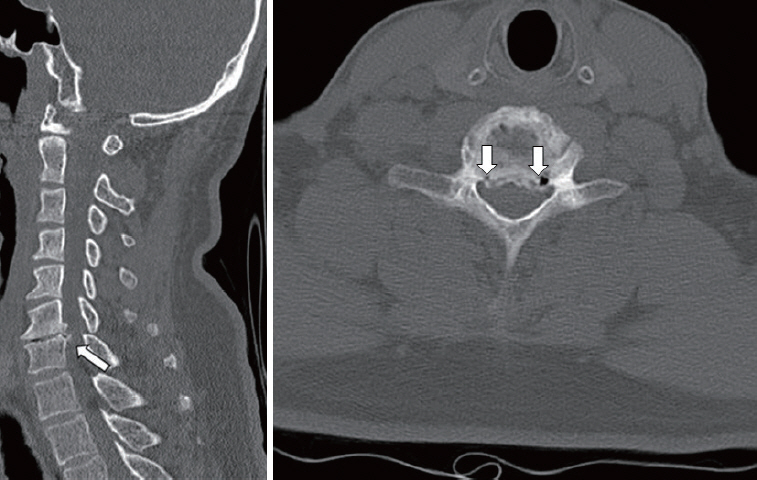
Fig. 1. Cervical computerized tomography scan showing prominent both foraminal stenosis (axial image white arrow) and uncovertebral joint hypertrophy (sagittal image white arrow).
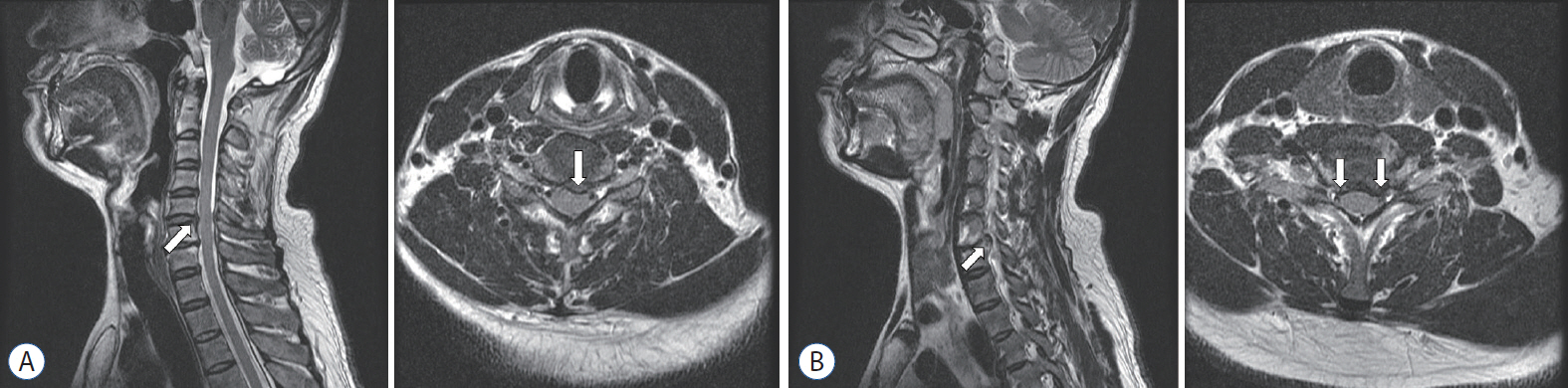
Fig. 2. A : Magnetic resonance imaging (MRI) revealing mild disc protrusion at the C5–6 disc level (white arrow). B : Preoperative MRI showing both foraminal stenosis at the C6–7 disc level (white arrow).
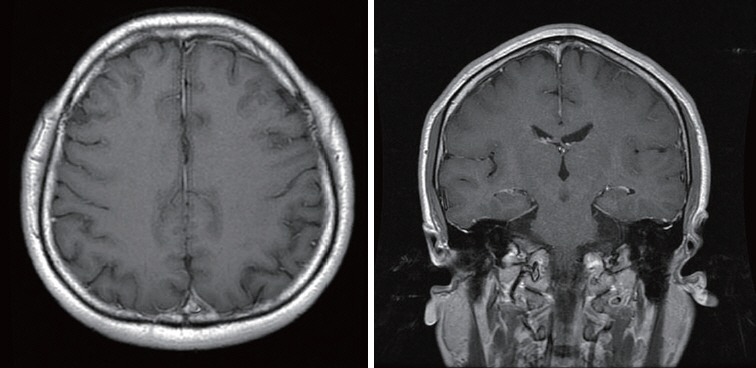
Fig. 3. Normal brain magnetic resonance imaging taken 2 years before the symptoms occurred.
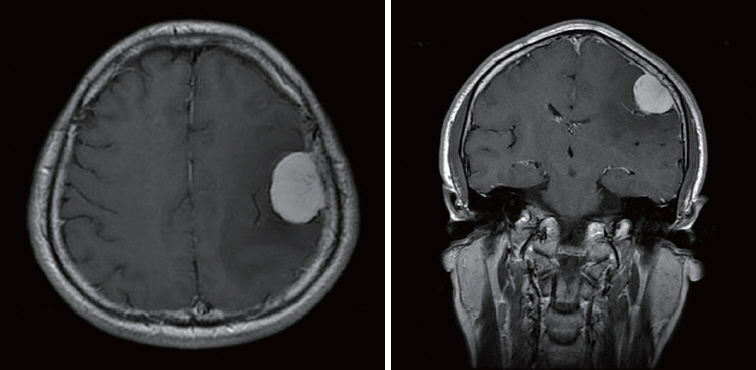
Fig. 4. New brain mass found on brain magnetic resonance imaging taken 1 week after cervical operation.

Fig. 5. Degenerative change and protrusion of cervical disc (C5–6 level) having a compressive effect on spinal cord.

Fig. 6. Computerized tomography myelogram suggestive of left foraminal stenosis at C5–6 level due to bony spur (white arrow).

Fig. 7. Postoperative magnetic resonance images showing decompressed cervical C5–6 level but slight narrowing of the left foramen.
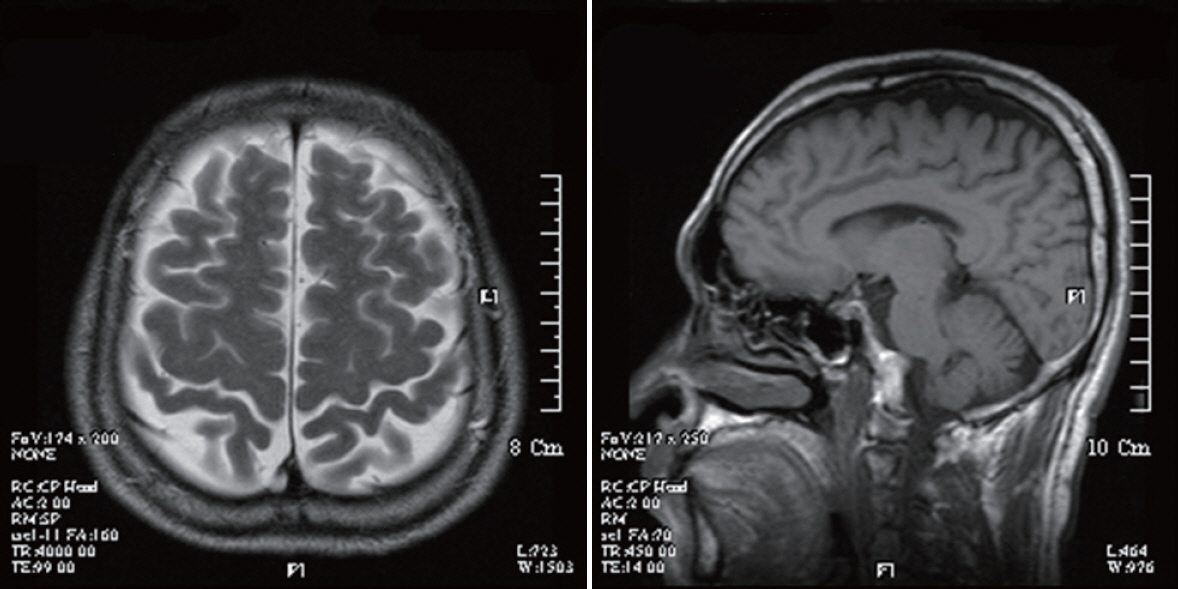
Fig. 8. Normal brain magnetic resonance imaging taken 15 months prior to admission to our hospital.

Fig. 9. A : A simple chest X-ray showing a large mass on the left upper lung (white arrow). B : A chest computerized tomography scan confirms a large mass on the left upper lung (white arrow).

Fig. 10. New brain mass found on brain magnetic resonance imaging.
Reference
-
References
1. Caridi JM, Pumberger M, Hughes AP. Cervical radiculopathy: a review. HSS J. 7:265–272. 2011.
Article2. Clar SA, Cianca JC. Intracranial tumor masquerading as cervical radiculopathy: a case study. Arch Phys Med Rehabil. 79:1301–1302. 1998.
Article3. Huang YH, Hong CZ, Wu WT, Li KT, Chou LW. Brain meningioma with initial manifestation similar to cervical radiculopathy: a case report. Neuropsychiatr Dis Treat. 10:1175–1181. 2014.4. Khalatbari M, Ghalenoui H, Yahyavi ST, Borghei-Razavi H. Left somatosensory cortex tumor presented with radicular hand pain and paresthesia. Arch Iran Med. 11:107–109. 2008.5. Lim TH, Choi SI, Yoo JI, Choi YS, Lim YS, Sang BH, et al. Thalamic pain misdiagnosed as cervical disc herniation. Korean J Pain. 29:119–122. 2016.
Article6. Makhni MC, Yeung CM, Riew KD. The art of diagnosis in the cervical spine. Neurospine. 17:695–703. 2020.
Article7. Wainner RS, Gill H. Diagnosis and nonoperative management of cervical radiculopathy. J Orthop Sports Phys Ther. 30:728–744. 2000.
Article8. Wilson JRF, Badhiwala JH, Moghaddamjou A, Martin AR, Fehlings MG. Degenerative cervical myelopathy; a review of the latest advances and future directions in management. Neurospine. 16:494–505. 2019.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Brain Tumor Mimicking Cervical Spinal Disease: A Case Report
- Cervical Radiculopathy Focus on Characteristics and Differential Diagnosis
- Cervical Radiculopathy due to Cervical Degenerative Diseases : Anatomy, Diagnosis and Treatment
- Diabetic Cervical Radiculopathy with Adhesive Capsulitis of the Shoulder
- Management of Cervical Radiculopathy with Epidural Steroid Injection
