Negative-Pressure Wound Therapy for Septic Ankle Arthritis Following Intractable Lateral Malleolar Bursitis: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, Kosin University College of Medicine, Busan, Korea
- KMID: 2523302
- DOI: http://doi.org/10.14193/jkfas.2021.25.4.190
Abstract
- A bursa is an obstructive sac filled with synovial fluid and usually occurs in any area of the body exposed to friction. The bursa of the ankle is not a normal anatomical structure and is caused by repetitive trauma, constant friction, or inflammatory disease of the ankle. Bursitis can occur in any bursa in the human body; however it rarely progresses to septic arthritis. We report a rare case of septic ankle arthritis following intractable lateral malleolar bursitis successfully treated with negative-pressure wound therapy.
Figure
-

Figure. 1 Gross images (A, B) of left lateral malleolar bursitis at initial visit. There was an about 1-cm sized wound opening with pus-like discharge. Anteroposterior radiograph of both ankle joints (C) and lateral radiograph of left ankle joint (D) at initial visit. It showed soft tissue swelling around the left ankle joint without osteolytic bone lesion.
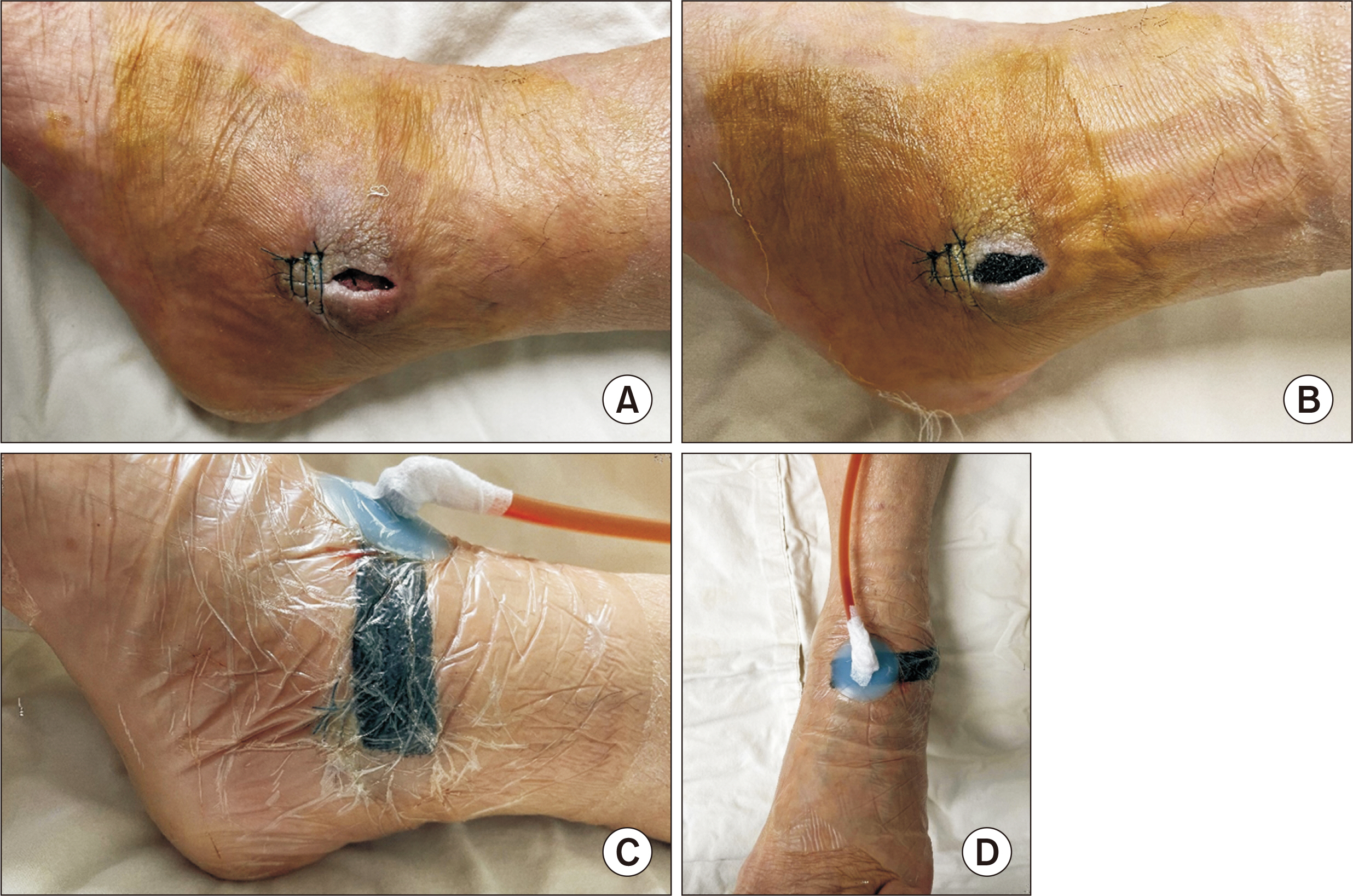
Figure. 2 Intraoperative gross images at 3 days after the initial operation in our hospital. (A) The wound was sutured only from the distal 1/2 of the wound with the proximal part of the wound open for negative pressure wound therapy. (B) The interface material (foam) was cut to be smaller than the width of the wound because the area around the wound easily macerated. (C, D) The suction head was positioned forward rather than lateral side of the ankle joint to prevent chronic pressure on the lateral malleolus.

Figure. 3 Coronal T2 (A), axial T1 (B), and sagittal T2 (C) -weighted magnetic resonance images showing joint effusion with synovial enhancement and normal signal intensity of bone. Three phase bone scan (D) shows increased uptake with hyperemia of the left ankle joint.

Figure. 4 Arthroscopic finding showed hypertrophic synovial membrane on the posterior (A) and lateral (B) ankle joint. Because the ankle joint communicated with the outside through the wound, a non-absorbable suture was used on the front of the distal fibula from the skin to the periosteum (C).

Figure. 5 Gross images of left lateral malleolus at 4 weeks (A) and 5 weeks (B) after the initial operation at our hospital. (B) At 5 weeks, granulation tissue was formed in the wound and the wound was completely closed with non-absorbable sutures. (C) Gross image shows complete healing of the wound at 6-month follow-up.
Reference
-
References
1. Brown TD, Varney TE, Micheli LJ. 2000; Malleolar bursitis in figure skaters. Indications for operative and nonoperative treatment. Am J Sports Med. 28:109–11. doi: 10.1177/03635465000280010301. DOI: 10.1177/03635465000280010301. PMID: 10653553.2. Larsson LG, Baum J. 1986; The syndromes of bursitis. Bull Rheum Dis. 36:1–8. PMID: 3790856.3. Boutin FJ BR, Boutin FJ Jr. Chapman MW, Madison M, editors. 1993. Bursitis. Operative orthopaedics. 2nd ed. JB Lippincott Co;Philadelphia: p. 3419–32.4. Hernandez PA, Hernandez WA, Hernandez A. 1991; Clinical aspects of bursae and tendon sheaths of the foot. J Am Podiatr Med Assoc. 81:366–72. doi: 10.7547/87507315-81-7-366. DOI: 10.7547/87507315-81-7-366. PMID: 1941580.
Article5. Woo SH, Kim JS, Son SM, Shin WC. 2019; Triamcinolone acetonide injections for lateral malleolar bursitis of the ankle. J Korean Foot Ankle Soc. 23:12–7. doi: 10.14193/jkfas.2019.23.1.12. DOI: 10.14193/jkfas.2019.23.1.12.
Article6. Weston V, Coakley G. 2006; Guideline for the management of the hot swollen joint in adults with a particular focus on septic arthritis. J Antimicrob Chemother. 58:492–3. doi: 10.1093/jac/dkl295. DOI: 10.1093/jac/dkl295. PMID: 16857687.
Article7. Vispo Seara JL, Barthel T, Schmitz H, Eulert J. 2002; Arthroscopic treatment of septic joints: prognostic factors. Arch Orthop Trauma Surg. 122:204–11. doi: 10.1007/s00402-001-0386-z. DOI: 10.1007/s00402-001-0386-z. PMID: 12029509.8. Argenta LC, Morykwas MJ. 1997; Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg. 38:563–76. discussion 577doi: 10.1097/00000637-199706000-00002. DOI: 10.1097/00000637-199706000-00002. PMID: 9188971.9. Kim BS, Choi WJ, Baek MK, Kim YS, Lee JW. 2011; Limb salvage in severe diabetic foot infection. Foot Ankle Int. 32:31–7. doi: 10.3113/FAI.2011.0031. DOI: 10.3113/FAI.2011.0031. PMID: 21288432.
Article10. Birke-Sorensen H, Malmsjo M, Rome P, Hudson D, Krug E, Berg L, et al. Evidence-based recommendations for negative pressure wound therapy: treatment variables (pressure levels, wound filler and contact layer)--steps towards an international consensus. J Plast Reconstr Aesthet Surg. 2011; 64 Suppl:S1–16. doi: 10.1016/j.bjps.2011.06.001. DOI: 10.1016/j.bjps.2011.06.001. PMID: 21868296.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Secondary Septic Arthritis Due to Lateral Malleolar Bursitis: A Case Report
- Surgery for Synovial Fistula after Excision of the Lateral Malleolar Bursitis of the Ankle: A Case Report
- Outcomes of Lateral Malleolar Saving versus Sacrificing Procedure in Transfibular Ankle Arthrodesis
- Endoscopy versus Open Bursectomy of Lateral Malleolar Bursitis; Comparative Study
- The Effect of Indwelling Silk Suture Following Aspiration in the Treatment of Chronic Lateral Malleolar Bursitis
