Transnasal Endoscopic Resection of a Huge Solitary Fibrous Tumor Originated From Frontal Recess
- Affiliations
-
- 1Department of Otorhinolaryngology, Gyeongsang National University School of Medicine, Gyeongsang National University Hospital, Jinju, Republic of Korea
- 2Institute of Health Sciences, Gyeongsang National University, Jinju, Republic of Korea
- KMID: 2522787
- DOI: http://doi.org/10.18787/jr.2021.00347
Abstract
- Solitary fibrous tumor (SFT) is a spindle cell neoplasm that occurs commonly in the pleural space. One-third of SFTs arising from an extrathoracic organ are found in the head and neck region, and they arise rarely in the sinonasal tract. Most of these tumors are benign, but malignant tumors are identified in some cases. Here we report a rare sinonasal SFT arising from the frontal recess. A 32-year-old male patient with chief complaint of headache and left facial pain visited the outpatient clinic. He had suffered from paranasal pain and nasal obstruction for several months, and symptoms became more severe in the previous three months. The mass rapidly increased in size and was protruding from the left nostril when he visited the hospital. After computed tomography and magnetic resonance imaging scans, transnasal endoscopic resection of the tumor was performed, and gross total tumor removal was successfully achieved. We believe this case will be helpful for providing information regarding management of such uncommon huge sinonasal tumors originating from the frontal recess.
Figure
-
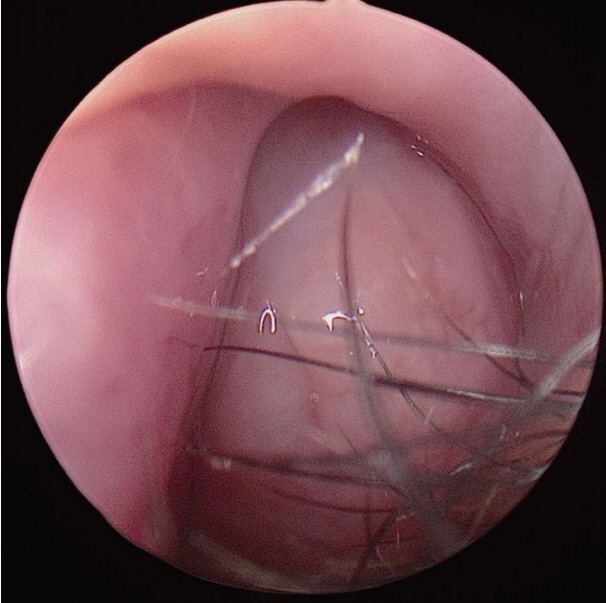
Fig. 1. A smooth white mass occupying the entire left nasal cavity found in rigid nasal endoscopy.
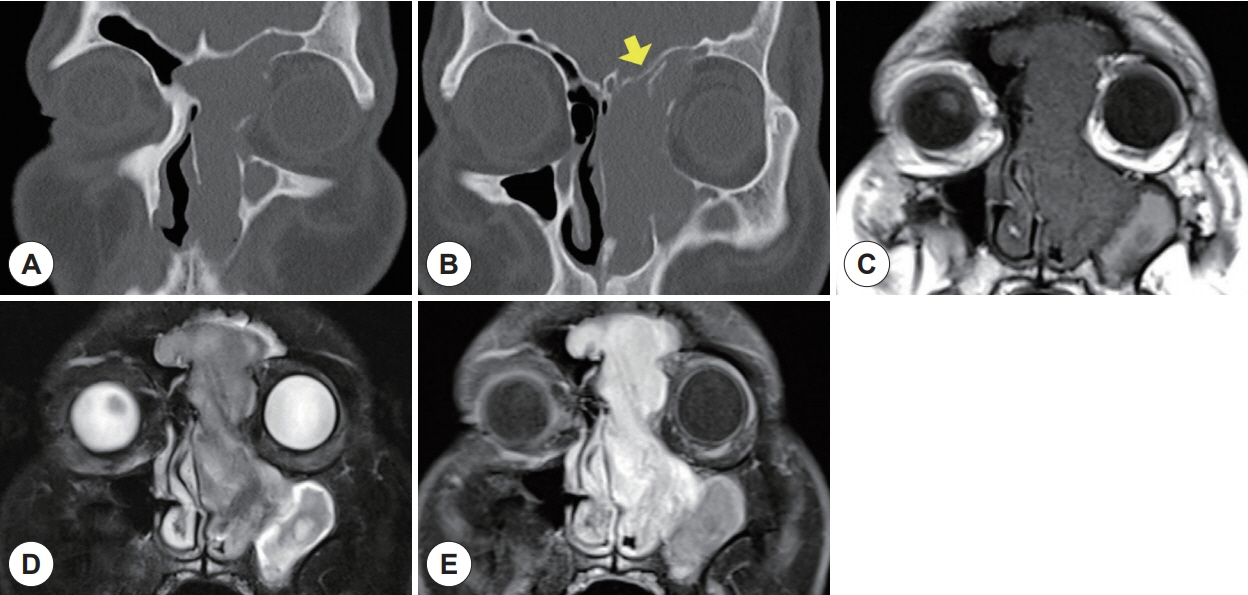
Fig. 2. A huge heterogeneous enhancing mass with high vascularity in left nasal cavity, maxillary sinus, ethmoid sinus, and both frontal sinuses was found in paranasal sinus CT (A, B) and T1-weighted, T2-weighted and T1-enhanced MRI (C, D, E). The suspicious origin site was frontal recess, and it was labeled by an arrow.
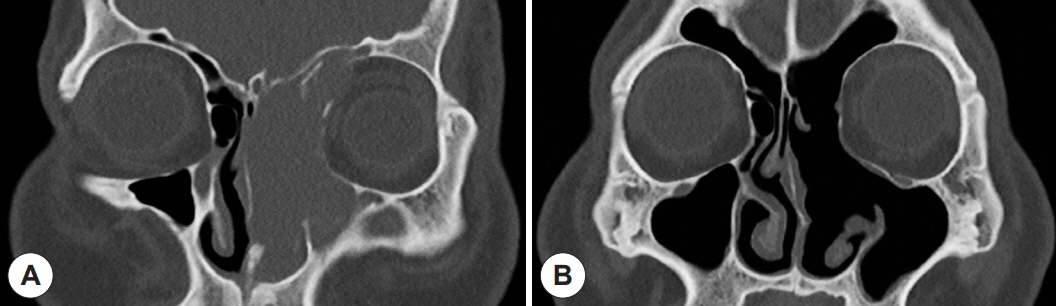
Fig. 3. (A) Preoperative and (B) postoperative paranasal CT image finding (coronal plane) of the patient with paranasal SFT. The tumor was successfully excised by transnasal endoscopic approach.
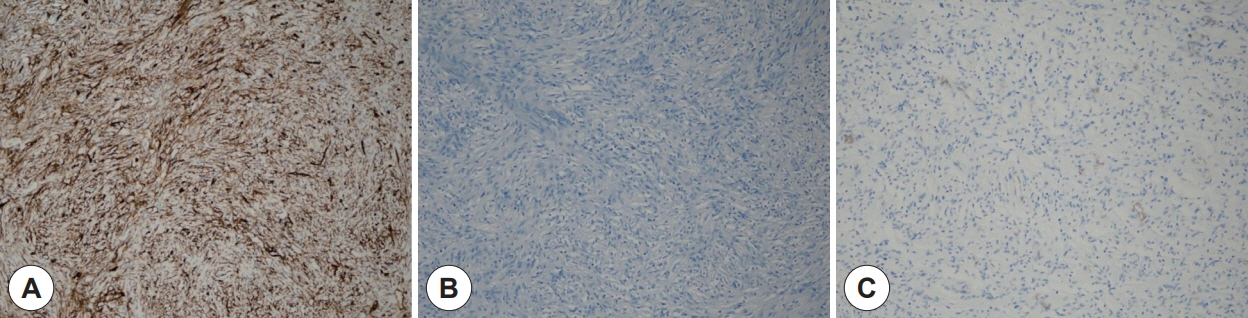
Fig. 4. Immunohistochemical stainings of the paranasal sinus tumor were performed to diagnose solitary fibrous tumor. (A) positive for CD34, (B) negative for S100 and (C) SMA (100× magnification).
Reference
-
References
1. Klemperer P, Rabin C. Primary neoplasms of the pleura. A report of five cases. Arch Pathol. 1931; 11:385–412.2. Stout AP, Himadi GM. Solitary (localized) mesothelioma of the pleura. Ann Surg. 1951; 133(1):50–64.3. Dunfee BL, Sakai O, Spiegel JH, Pistey R. Solitary fibrous tumor of the buccal space. AJNR Am J Neuroradiol. 2005; 26(8):2114–6.4. Nielsen GP, O’Connell JX, Dickersin GR, Rosenberg AE. Solitary fibrous tumor of soft tissue: a report of 15 cases, including 5 malignant examples with light microscopic, immunohistochemical, and ultrastructural data. Mod Pathol. 1997; 10(10):1028–37.5. Takasaki K, Watanabe T, Hayashi T, Kinoshita N, Kumagami H, Takahashi H. Solitary fibrous tumor arising from the sphenoid sinus. Case Rep Med. 2009; 2009:316042.6. Mathew GA, Ashish G, Tyagi AK, Chandrashekharan R, Paul RR. Solitary fibrous tumor of nasal cavity: a case report. Iran J Otorhinolaryngol. 2015; 27(81):307–12.7. Zeitler DM, Kanowitz SJ, Har-El G. Malignant solitary fibrous tumor of the nasal cavity. Skull Base. 2007; 17(4):239–46.8. Zielińska-Kaźmierska B, Grodecka J, Szyszkowski A. Solitary fibrous tumor of the nasal cavity and paranasal sinuses: a case report. J Oral Biol Craniofac Res. 2015; 5(2):112–6.9. Ahn TJ, Bae WY, Kim SJ, Kang MJ. Solitary fibrous tumor in nasal cavity: surgical treatment after angiographic embolization. Korean J Otorhinolaryngol-Head Neck Surg. 2009; 52(3):258–61.10. Kim JH, Yim JW, Kim HK, Lee JG. A case of solitary fibrous tumor of the nasal cavity. J Rhinol. 2003; 10(1, 2):60–3.11. Kodama S, Fujita K, Suzuki M. Solitary fibrous tumor in the maxillary sinus treated by endoscopic medial maxillectomy. Auris Nasus Larynx. 2009; 36(1):100–3.12. Hasegawa T, Matsuno Y, Shimoda T, Hasegawa F, Sano T, Hirohashi S. Extrathoracic solitary fibrous tumors: their histological variability and potentially aggressive behavior. Hum Pathol. 1999; 30(12):1464–73.13. Kohmura T, Nakashima T, Hasegawa Y, Matsuura H. Solitary fibrous tumor of the paranasal sinuses. Eur Arch Otorhinolaryngol. 1999; 256(5):233–6.14. Thompson LDR, Lau SK. Sinonasal tract solitary fibrous tumor: a clinicopathologic study of six cases with a comprehensive review of the literature. Head Neck Pathol. 2018; 12(4):471–80.15. Goodlad JR, Fletcher CD. Solitary fibrous tumour arising at unusual sites: analysis of a series. Histopathology. 1991; 19(6):515–22.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Frontal Sinus Surgery
- Resection of Impacted Bilateral Huge Frontal Osteoma Via Endoscopic Modified Lothrop Approach
- A Huge Osteoma Originated From the Frontal Sinus: Case Report
- A Case of Treatment of Traumatic Recurrent Frontal Sinusitis with T-tube
- Acute Frontal Osteomyelitis Managed by Endoscopic Sinus Surgery: A Case Report
