Cardiopulmonary bypass preparation is mandatory in cardiac exploration for blunt cardiac injury patients: two case reports
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, School of Medicine, Kyungpook National University, Kyungpook National University Hospital, Daegu, Korea
- KMID: 2521716
- DOI: http://doi.org/10.12701/yujm.2020.00822
Abstract
- Treating cardiac injuries following blunt trauma to the chest requires thorough examination, accurate diagnosis, and therapeutic plan. We present two cases; pulmonary vein rupture and left atrial appendage laceration, both as a result of blunt chest trauma. Through these cases, our team learned the importance of maintaining hemodynamic stability during the examination of injured cardiac structures. And based on the comprehensive cardiac examination, a decision to surgically intervene with median sternotomy via cardiopulmonary bypass was made, saving lives of the patient. This report introduces how such decision was made based on what supporting evidence and the diagnostic process leading to the initiation of surgical intervention. This report may help with decision-making process when confronted by blunt cardiac injury patients who need cardiac exploration.
Figure
-
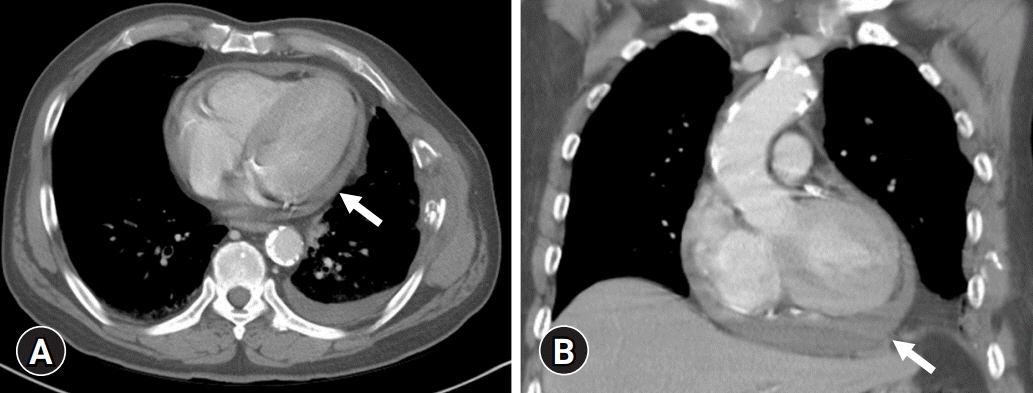
Fig. 1. Initial chest computed tomography (CT) scan of case 1. (A) Initial chest CT scan shows a small amount of hemopericardium (arrow), scanty left hemothorax, and rib fractures. (B) Coronal view of the chest CT scan reveals a small amount of hemopericardium (arrow) and aortic calcifications.
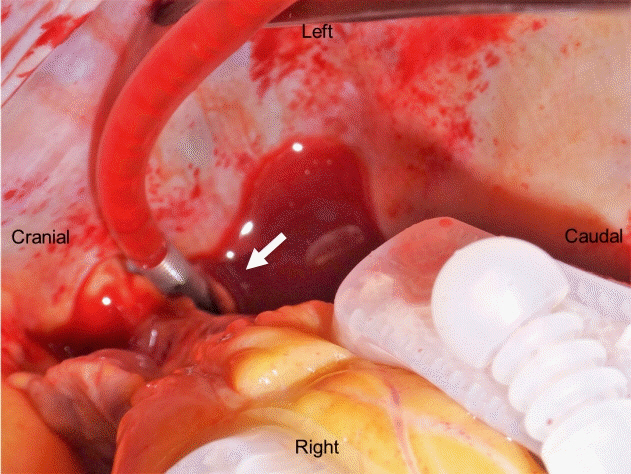
Fig. 2. Perioperative findings in case 1. Operative view shows a 2-cm rupture of the left upper pulmonary vein at its junction with the left atrium (arrow). This tear can be revealed in the bloodless field and decompressed heart using cardiopulmonary bypass.
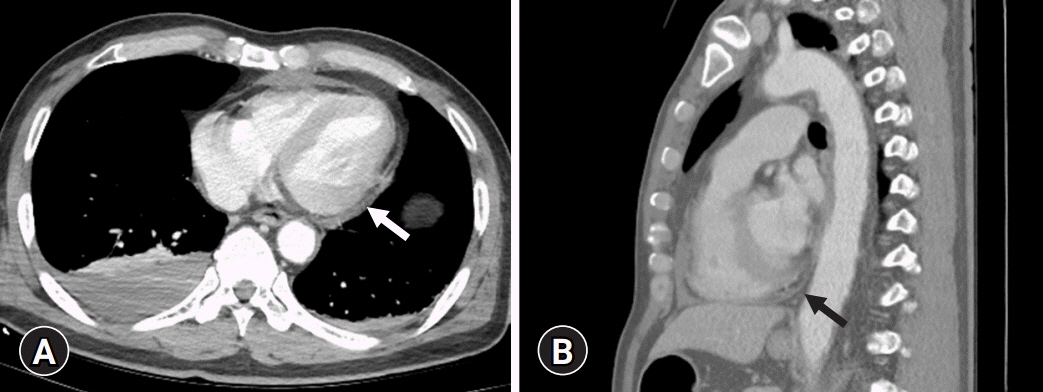
Fig. 3. Initial chest computed tomography (CT) scan of case 2. (A) Initial chest CT scan shows scanty hemopericardium (arrow) and right pleural effusion. We suspected right ventricle (RV) injury due to hematoma between the RV and the sternum. (B) Sagittal view of the chest CT scan reveals a small hemopericardium (arrow).
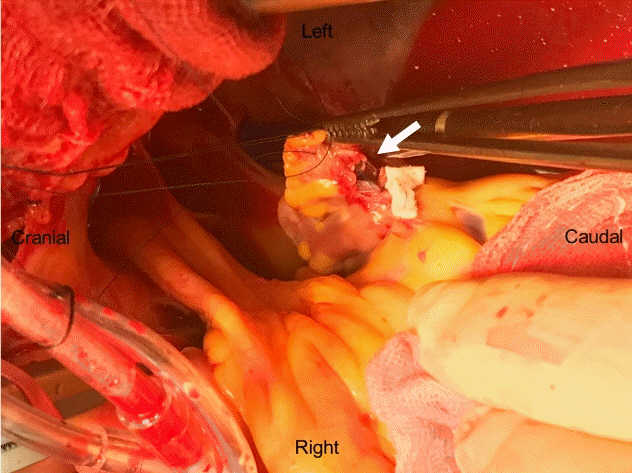
Fig. 4. Perioperative findings in case 2. Operative view shows a 1.5-cm rupture of the left atrium appendage (arrow). We repaired the appendage laceration using 4-0 polypropylene suture with polytetrafluoroethylene felt pledget reinforcement, carefully avoiding the left circumflex artery.
Reference
-
References
1. Teixeira PG, Inaba K, Oncel D, DuBose J, Chan L, Rhee P, et al. Blunt cardiac rupture: a 5-year NTDB analysis. J Trauma. 2009; 67:788–91.
Article2. Turk EE, Tsang YW, Champaneri A, Pueschel K, Byard RW. Cardiac injuries in car occupants in fatal motor vehicle collisions: an autopsy-based study. J Forensic Leg Med. 2010; 17:339–43.3. Hawkins ML, Carraway RP, Ross SE, Johnson RC, Tyndal EC, Laws HL. Pulmonary artery disruption from blunt thoracic trauma. Am Surg. 1988; 54:148–52.4. Turan AA, Karayel FA, Akyildiz E, Pakis I, Uzun I, Gurpinar K, et al. Cardiac injuries caused by blunt trauma: an autopsy based assessment of the injury pattern. J Forensic Sci. 2010; 55:82–4.
Article5. Teixeira PG, Inaba K, Barmparas G, Georgiou C, Toms C, Noguchi TT, et al. Blunt thoracic aortic injuries: an autopsy study. J Trauma. 2011; 70:197–202.
Article6. Ouda A, Kappert U, Ghazy T, Weise M, Ebner B, Tugtekin SM, et al. Isolated rupture of the right upper pulmonary vein: a blunt cardiac trauma case. Ann Thorac Surg. 2011; 91:1267–9.
Article7. Yousef R, Carr JA. Blunt cardiac trauma: a review of the current knowledge and management. Ann Thorac Surg. 2014; 98:1134–40.
Article8. Le Guyader A, Bertin F, Laskar M, Cornu E. Blunt chest trauma: a right pulmonary vein rupture. Eur J Cardiothorac Surg. 2001; 20:1054–6.
Article9. Osaka M, Nagai R, Koishizawa T. Rupture of the right upper pulmonary vein and left atrium caused by blunt chest trauma. Gen Thorac Cardiovasc Surg. 2017; 65:646–9.
Article10. Nwaejike N, Mosca R, Hooper TL, Soon SY. Surgical repair of pulmonary vein injury from blunt trauma. Ann R Coll Surg Engl. 2015; 97:e34–6.
Article11. Varghese D, Patel H, Cameron EW, Robson M. Repair of pulmonary vein rupture after deceleration injury. Ann Thorac Surg. 2000; 70:656–8.
Article12. Fukunaga N, Konishi Y, Murashita T, Yuzaki M, Shomura Y, Koyama T, et al. Survival after simultaneous repair of bichamber cardiac and pulmonary vein rupture caused by blunt chest trauma. Ann Thorac Surg. 2012; 94:265–7.
Article13. Nan YY, Lu MS, Liu KS, Huang YK, Tsai FC, Chu JJ, et al. Blunt traumatic cardiac rupture: therapeutic options and outcomes. Injury. 2009; 40:938–45.
Article14. Brathwaite CE, Rodriguez A, Turney SZ, Dunham CM, Cowley R. Blunt traumatic cardiac rupture: a 5-year experience. Ann Surg. 1990; 212:701–4.
Article15. Fulda G, Brathwaite CE, Rodriguez A, Turney SZ, Dunham CM, Cowley RA. Blunt traumatic rupture of the heart and pericardium: a ten-year experience (1979-1989). J Trauma. 1991; 31:167–73.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatment of Blunt Traumatic Cardiac Rupture: Two Case Reports
- Acute Myocardial Infarction caused by Left Coronary Artery Aneurysm following Blunt Chest Trauma: A case report
- Application of Percutaneous Cardiopulmonary Support for Cardiac Tamponade Following Blunt Chest Trauma: Two Case Reports
- Cardiac Rupture of the Junction of the Right Atrium and Superior Vena Cava in Blunt Thoracic Trauma
- Cardiac Rupture after Blunt Chest Trauma
