Prognostic impact of chromogranin A in patients with acute heart failure
- Kim HN
 1,2
1,2 - Yang DH1,2,3
- Park BE1
- Park YJ1
- Kim HJ1
- Jang SY1,2,3
- Bae MH1,3
- Lee JH1,3
- Park HS1,3
- Cho Y1,3
- Chae SC1,3
- Affiliations
-
- 1Department of Internal Medicine, Kyungpook National University Hospital, Daegu, Korea
- 2Cardiology Center, Kyungpook National University Chilgok Hospital, Daegu, Korea
- 3Department of Internal Medicine, School of Medicine, Kyungpook National University, Daegu, Korea
- KMID: 2521713
- DOI: http://doi.org/10.12701/yujm.2020.00843
Abstract
- Background
Chromogranin A (CgA) levels have been reported to predict mortality in patients with heart failure. However, information on the prognostic value and clinical availability of CgA is limited. We compared the prognostic value of CgA to that of previously proven natriuretic peptide biomarkers in patients with acute heart failure.
Methods
We retrospectively evaluated 272 patients (mean age, 68.5±15.6 years; 62.9% male) who underwent CgA test in the acute stage of heart failure hospitalization between June 2017 and June 2018. The median follow-up period was 348 days. Prognosis was assessed using the composite events of 1-year death and heart failure hospitalization.
Results
In-hospital mortality rate during index admission was 7.0% (n=19). During the 1-year follow-up, a composite event rate was observed in 12.1% (n=33) of the patients. The areas under the receiver-operating characteristic curves for predicting 1-year adverse events were 0.737 and 0.697 for N-terminal pro-B-type natriuretic peptide (NT-proBNP) and CgA, respectively. During follow-up, patients with high CgA levels (>158 pmol/L) had worse outcomes than those with low CgA levels (≤158 pmol/L) (85.2% vs. 58.6%, p<0.001). When stratifying the patients into four subgroups based on CgA and NT-proBNP levels, patients with high NT-proBNP and high CgA had the worst outcome. CgA had an incremental prognostic value when added to the combination of NT-proBNP and clinically relevant risk factors.
Conclusion
The prognostic power of CgA was comparable to that of NT-proBNP in patients with acute heart failure. The combination of CgA and NT-proBNP can improve prognosis prediction in these patients.
Keyword
Figure
-
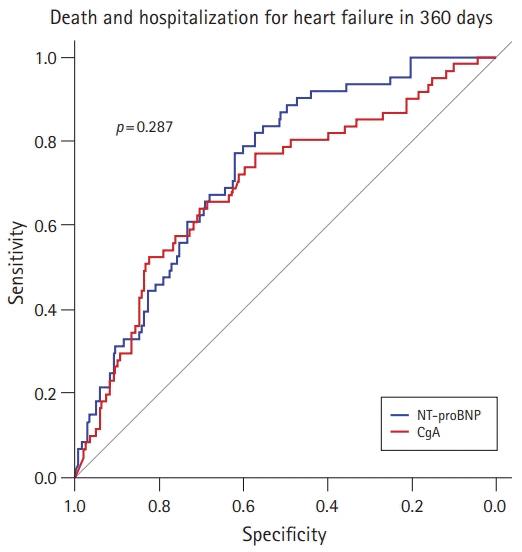
Fig. 1. Receiver-operating characteristic curve analysis of N-terminal pro-B-type natriuretic peptide (NT-proBNP) and chromogranin A (CgA) in predicting the composite outcome of 1-year death and hospitalization for heart failure. The cutoff values for CgA and NT-proBNP were 158 pmol/L and 3,429 pg/mL, respectively. Areas under the curves for CgA and NT-proBNP levels in predicting 1-year death and hospitalization were 0.697 and 0.737, respectively.

Fig. 2. Kaplan-Meier survival analysis of the groups according to the levels of chromogranin A (CgA; cutoff value=158 pmol/L) and N-terminal pro-B-type natriuretic peptide (NT-proBNP; cutoff value=3,429 pg/mL).
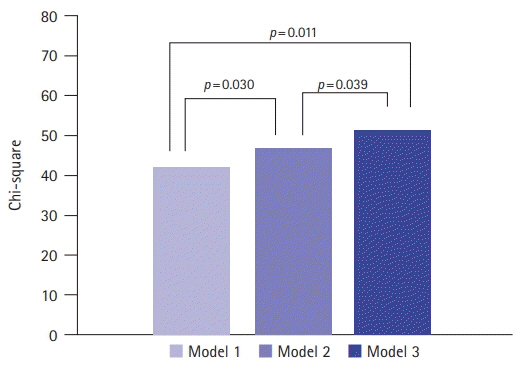
Fig. 3. Comparison among the models including the established risk factors, N-terminal pro-B-type natriuretic peptide (NT-proBNP), and chromogranin A (CgA) in predicting 1-year mortality. Model 1 includes age, sex, New York Heart Association (NYHA) class, atrial fibrillation, and de novo heart failure. Model 2: model 1+NT-proBNP. Model 3: model 2+CgA.
Reference
-
References
1. Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation. 2019; 139:e56–528.2. Lee SE, Lee HY, Cho HJ, Choe WS, Kim H, Choi JO, et al. Clinical characteristics and outcome of acute heart failure in Korea: results from the Korean Acute Heart Failure Registry (KorAHF). Korean Circ J. 2017; 47:341–53.
Article3. Ahn MS, Yoo BS, Yoon J, Lee SH, Kim JY, Ahn SG, et al. Prognostic effect of guideline-directed therapy is more noticeable early in the course of heart failure. J Korean Med Sci. 2019; 34:e133.
Article4. Kim MS, Lee JH, Kim EJ, Park DG, Park SJ, Park JJ, et al. Korean Guidelines for Diagnosis and Management of Chronic Heart Failure. Korean Circ J. 2017; 47:555–643.
Article5. Lee JH, Kim MS, Yoo BS, Park SJ, Park JJ, Shin MS, et al. KSHF Guidelines for the Management of Acute Heart Failure: Part II. Treatment of acute heart failure. Korean Circ J. 2019; 49:22–45.
Article6. Lee JH, Kim MS, Kim EJ, Park DG, Cho HJ, Yoo BS, et al. KSHF Guidelines for the Management of Acute Heart Failure: Part I. Definition, epidemiology and diagnosis of acute heart failure. Korean Circ J. 2019; 49:1–21.
Article7. Cryer PE, Wortsman J, Shah SD, Nowak RM, Deftos LJ. Plasma chromogranin A as a marker of sympathochromaffin activity in humans. Am J Physiol. 1991; 260(2 Pt 1):E243–6.
Article8. Eriksson B, Arnberg H, Oberg K, Hellman U, Lundqvist G, Wernstedt C, et al. Chromogranins: new sensitive markers for neuroendocrine tumors. Acta Oncol. 1989; 28:325–9.9. Jansson AM, Røsjø H, Omland T, Karlsson T, Hartford M, Flyvbjerg A, et al. Prognostic value of circulating chromogranin A levels in acute coronary syndromes. Eur Heart J. 2009; 30:25–32.
Article10. Ceconi C, Ferrari R, Bachetti T, Opasich C, Volterrani M, Colombo B, et al. Chromogranin A in heart failure; a novel neurohumoral factor and a predictor for mortality. Eur Heart J. 2002; 23:967–74.
Article11. Ottesen AH, Carlson CR, Louch WE, Dahl MB, Sandbu RA, Johansen RF, et al. Glycosylated chromogranin A in heart failure: implications for processing and cardiomyocyte calcium homeostasis. Circ Heart Fail. 2017; 10:e003675.12. Estensen ME, Hognestad A, Syversen U, Squire I, Ng L, Kjekshus J, et al. Prognostic value of plasma chromogranin A levels in patients with complicated myocardial infarction. Am Heart J. 2006; 152:927.
Article13. Røsjø H, Masson S, Latini R, Flyvbjerg A, Milani V, La Rovere MT, et al. Prognostic value of chromogranin A in chronic heart failure: data from the GISSI-Heart Failure trial. Eur J Heart Fail. 2010; 12:549–56.
Article14. Kantar M, Levent E, Cetingul N, Ulger Z, Ozyurek R, Aksoylar S, et al. Plasma natriuretic peptides levels and echocardiographic findings in late subclinical anthracycline toxicity. Pediatr Hematol Oncol. 2008; 25:723–33.
Article15. Bhalla V, Willis S, Maisel AS. B-type natriuretic peptide: the level and the drug: partners in the diagnosis of congestive heart failure. Congest Heart Fail. 2004; 10(1 Suppl 1):3–27.
Article16. Huang B, Shen J, Li L, Huang Y, Luo S. Effect of B-type natriuretic peptide level on long-term outcome in patients with end-stage heart failure. Am J Cardiol. 2016; 118:383–8.
Article17. Kim MS, Lee JH, Cho HJ, Cho JY, Choi JO, Hwang KK, et al. KSHF Guidelines for the Management of Acute Heart Failure: Part III. Specific management of acute heart failure according to the etiology and co-morbidity. Korean Circ J. 2019; 49:46–68.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Elucidating the Interplay: Exploring the Impact of Acute Heart Failure on Aspiration Pneumonia Hospitalizations
- Elevating Right Ventricular Assessment: The Transformative Prognostic Power of RVGLS/PASP Ratio in Acute Heart Failure
- The Impact of COVID-19 on Heart Failure: What Happened to the Patients with Heart Failure Who Could Not Visit Our Clinic Amid the COVID-19 Pandemic?
- The Prognostic Significance of Neuroendocrine Differentiation for Treating Prostatic Carcinoma in 699 Cases of Radical Prostatectomy
- Effectiveness and Approach of Rehabilitation in Patients With Acute Heart Failure: A Review
