Pediatric Crohn’s disease with severe morbidity manifested by gastric outlet obstruction: two cases report and review of the literature
- Affiliations
-
- 1Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2521611
- DOI: http://doi.org/10.5217/ir.2020.00072
Abstract
- Crohn’s disease (CD) presenting as gastric outlet obstruction is rare but serious clinical presentation of CD causing severe morbidity. However, there have been few case reports concerning this disorder in East Asian children and adolescents. The current case report describes 2 pediatric patients with CD who had had gastric outlet obstruction as an initial symptom of CD. Two pediatric patients developed postprandial vomiting, bloating, and unintentional weight loss. The upper endoscopy result indicated that there was pyloric obstruction with mucosal edema, inflammation and ulcers. The serologic test and colonoscopy results suggested CD. These patients were treated with infliximab, and endoscopic balloon dilation without surgery and showed remarkable improvement in obstructing symptoms with maintaining clinical and biochemical remission. This case report elucidates the benefits of early intervention using infliximab and endoscopic balloon dilation to improve gastric outlet obstruction and achieve baseline recovery in patients with upper gastrointestinal B2 phenotype of CD.
Keyword
Figure
-
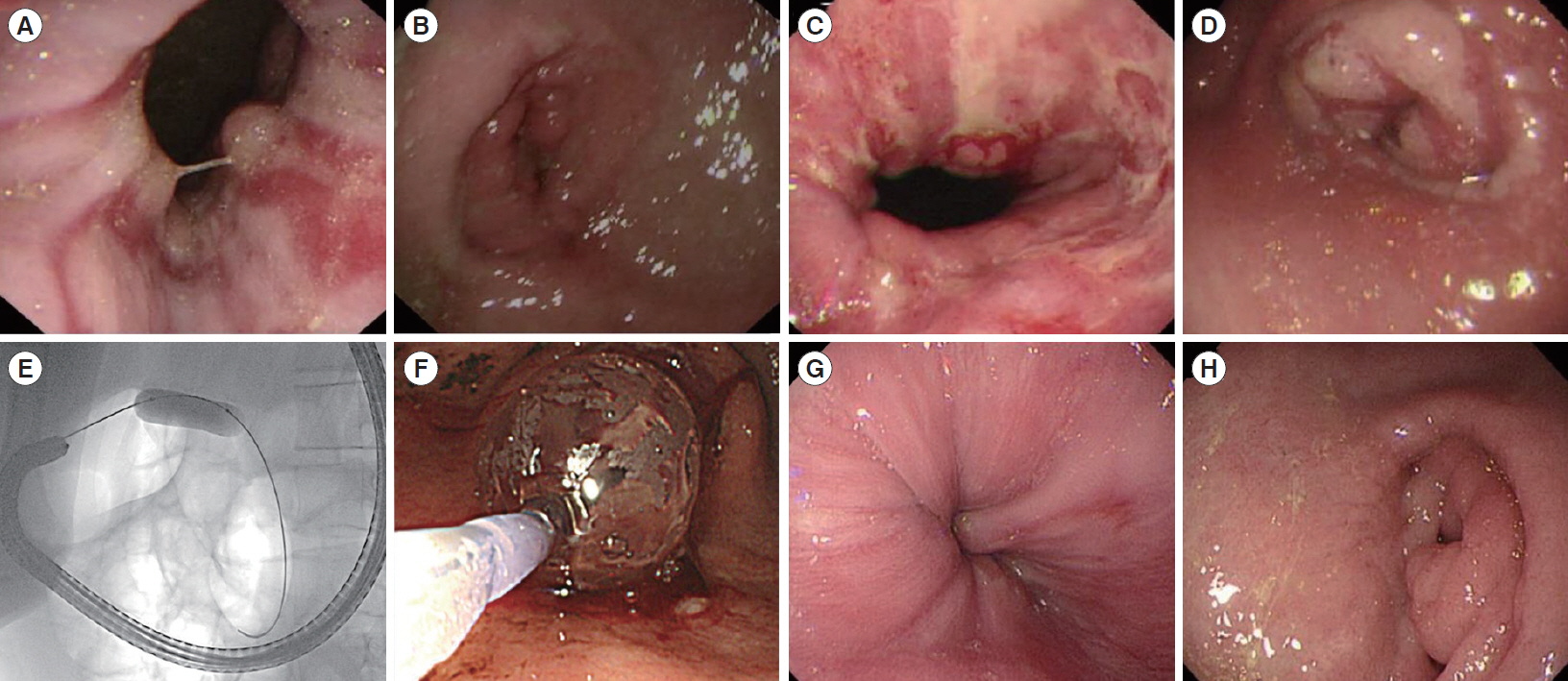
Fig. 1. Esophagogastroduodenoscopy at diagnosis (case 1). (A, B) Upper endoscopic findings at referral. Reflux esophagitis at low esophagus, multiple esophageal ulcers, and significant narrowing of pylorus. (C, D) Follow-up upper endoscopic findings after 11 weeks. Apparent pyloric obstruction and multiple ulcerations on antrum. (E, F) Fluoroscopically guided balloon dilation. (G, H) Follow-up upper endoscopic findings after 20 weeks. Remarkable improvement of reflux esophagitis and pyloric obstruction.

Fig. 2. Colonoscopy at referral (case 1). (A) Multiple erosions in terminal ileum. (B) Mild swelling in ileocecal valve.

Fig. 3. Histopathologic findings of cases. (A) Case 1: gastric biopsy specimens showing small clusters of lymphocytes in the lamina propria, also called as focally enhanced gastritis (H&E, ×4). (B) Case 1: terminal ileal biopsy specimens showing villous blunting, crypt distortion and increased lymphoplasmacytic infiltration (H&E, ×4). (C) Case 2: colonic biopsy specimens showing a shallow ulcerative lesion and increased lymphoplasmacytic infiltration in submucosal layer and lamina propria of mucosa (H&E, ×4).
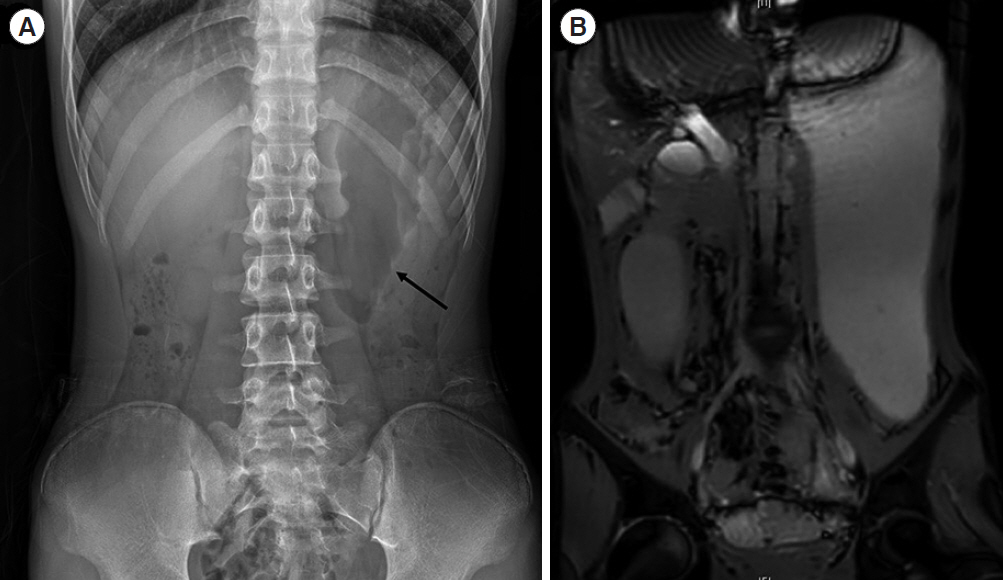
Fig. 4. Abdomen imaging at referral (case 1). (A) Plain X-ray revealed severe distended stomach (arrow) due to obstruction. (B) Magnetic resonance enterography revealed markedly distended stomach with gastric outlet obstruction, and limited evaluation of small bowel loops because of poor passage of contrast and collapse of small bowel.
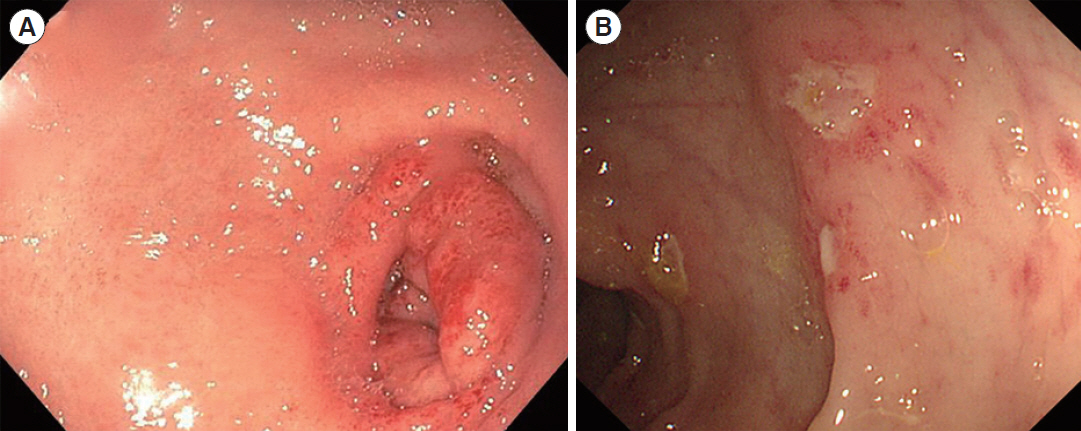
Fig. 5. Esophagogastroduodenoscopy and colonoscopy at referral (case 2). (A) Upper endoscopic findings at referral. Edematous mucosa, multiple pyloric ulcers, and significant narrowing of pylorus. (B) Several multiple aphthous ulcers in terminal ileum, and cecum to sigmoid colon.
Reference
-
1. Hyams JS. Inflammatory bowel disease. Pediatr Rev. 2005; 26:314–320.2. Benchimol EI, Fortinsky KJ, Gozdyra P, Van den Heuvel M, Van Limbergen J, Griffiths AM. Epidemiology of pediatric inflammatory bowel disease: a systematic review of international trends. Inflamm Bowel Dis. 2011; 17:423–439.3. Chouliaras G, Margoni D, Dimakou K, Fessatou S, Panayiotou I, Roma-Giannikou E. Disease impact on the quality of life of children with inflammatory bowel disease. World J Gastroenterol. 2017; 23:1067–1075.4. Cosnes J, Bourrier A, Nion-Larmurier I, Sokol H, Beaugerie L, Seksik P. Factors affecting outcomes in Crohn’s disease over 15 years. Gut. 2012; 61:1140–1145.
Article5. Horjus Talabur Horje CS, Meijer J, Rovers L, van Lochem EG, Groenen MJ, Wahab PJ. Prevalence of upper gastrointestinal lesions at primary diagnosis in adults with inflammatory bowel disease. Inflamm Bowel Dis. 2016; 22:1896–1901.6. Levine A, Koletzko S, Turner D, et al. ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J Pediatr Gastroenterol Nutr. 2014; 58:795–806.7. Abuquteish D, Putra J. Upper gastrointestinal tract involvement of pediatric inflammatory bowel disease: a pathological review. World J Gastroenterol. 2019; 25:1928–1935.
Article8. Tobin JM, Sinha B, Ramani P, Saleh AR, Murphy MS. Upper gastrointestinal mucosal disease in pediatric Crohn disease and ulcerative colitis: a blinded, controlled study. J Pediatr Gastroenterol Nutr. 2001; 32:443–448.9. Song XM, Gao X, Li MZ, et al. Clinical features and risk factors for primary surgery in 205 patients with Crohn’s disease: analysis of a South China cohort. Dis Colon Rectum. 2011; 54:1147–1154.
Article10. Inayat F, Ullah W, Hussain Q, Shafique K. Crohn’s disease presenting as gastric outlet obstruction: a therapeutic challenge? BMJ Case Rep. 2017; 2017–bcr2016218181.
Article11. Nugent FW, Roy MA. Duodenal Crohn’s disease: an analysis of 89 cases. Am J Gastroenterol. 1989; 84:249–254.12. Ho CH, Sinatra FR, Pietzak MM. A 9-year-old girl with poor weight gain and postprandial vomiting. Gastroenterology. 2015; 148:904–905.
Article13. Murray JJ, Schoetz DJ Jr, Nugent FW, Coller JA, Veidenheimer MC. Surgical management of Crohn’s disease involving the duodenum. Am J Surg. 1984; 147:58–65.
Article14. Yamamoto T, Fazio VW, Tekkis PP. Safety and efficacy of strictureplasty for Crohn’s disease: a systematic review and meta-analysis. Dis Colon Rectum. 2007; 50:1968–1986.
Article15. Tremaine WJ. Gastroduodenal Crohn’s disease: medical management. Inflamm Bowel Dis. 2003; 9:127–128.
Article16. Balendran K, Udumalagala S, Nawaraththne NMM. Pyloric stenosis as a manifestation of isolated gastric Crohn’s disease responding to intralesional steroid injection and balloon dilation: a case report. J Med Case Rep. 2019; 13:331.
Article17. Ibrahim SH, Smyrk TC, Faubion WA. Treatment of isolated gastric Crohn’s disease with inhaled corticosteroids. Case Rep Gastroenterol. 2008; 2:363–368.
Article18. Odashima M, Otaka M, Jin M, et al. Successful treatment of refractory duodenal Crohn’s disease with infliximab. Dig Dis Sci. 2007; 52:31–32.19. Gaggar S, Scott J, Thompson N. Pyloric stenosis associated Crohn’s disease responding to adalimumab therapy. World J Gastrointest Pharmacol Ther. 2012; 3:97–99.
Article20. Matsui T, Hatakeyama S, Ikeda K, Yao T, Takenaka K, Sakurai T. Long-term outcome of endoscopic balloon dilation in obstructive gastroduodenal Crohn’s disease. Endoscopy. 1997; 29:640–645.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Duodenal Crohn's Disease: A case report
- A Case of Congenital Gastric Outlet Obstruction with Serosal Fibrous Band in Prematurity
- Three Cases of Gastric Polyps Producing Intermittent Gastric Outlet Obstruction
- Eosinophilic gastroenteritis in a child with gastric outlet obstruction mimicking superior mesenteric artery syndrome
- A Man with Dysphagia after Cervical Esophagogastrostomy: A Case Report
