Self-expanding covered stent placement to treat a pseudoaneurysm caused by iatrogenic vertebral artery injury
- Affiliations
-
- 1Department of Neurosurgery, Penn State Health Milton S. Hershey Medical Center, PA, USA
- 2Department of Radiology, Penn State Health Milton S. Hershey Medical Center, PA, USA
- KMID: 2520887
- DOI: http://doi.org/10.7461/jcen.2021.E2021.03.006
Abstract
- Vertebral artery injuries account for approximately 19% of cerebral vascular injuries and are typically managed conservatively. However, some patients require operative intervention to gain control of an active hemorrhage, either via surgical ligation or endovascular intervention. We present a case of iatrogenic vertebral artery injury occurring during cervical spine surgery which was treated emergently with a self-expanding covered stent. A 58-year-old male presented for cervical traction, C5 and C6 corpectomy, and possible C4 to T2 posterior fusion following a motor vehicle accident. Intraoperatively, following drilling the C5 endplate, copious bleeding was observed from injury to the right vertebral artery resulting in pseudoaneurysm formation. The patient was loaded with ticagrelor and a self-expanding covered stent was placed via a transfemoral approach, resulting in obliteration of the pseudoaneurysm prior to completion of his cervical spine surgery. Emergent self-expanding covered stent placement for iatrogenic vertebral artery injury in the setting of an intraoperative injury is a safe and effective option. Ticagrelor is a viable alternative to traditional dual antiplatelet therapy for preventing thromboembolic complications in this urgent setting.
Figure
-
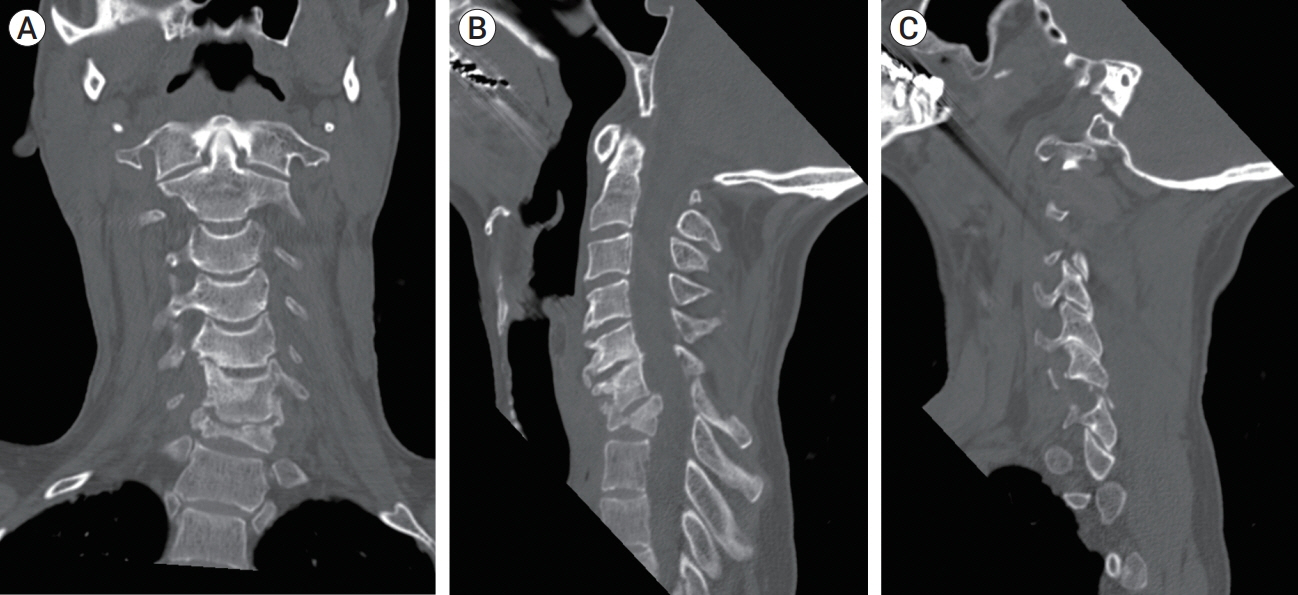
Fig. 1. Pre-operative computed tomography. Coronal view (A) revealed C7 burst fracture. Mid-sagittal view (B) revealed retropulsion of the burst segment into the spinal canal. Sagittal view (C) revealed C6 on C7 perched facet fractures.
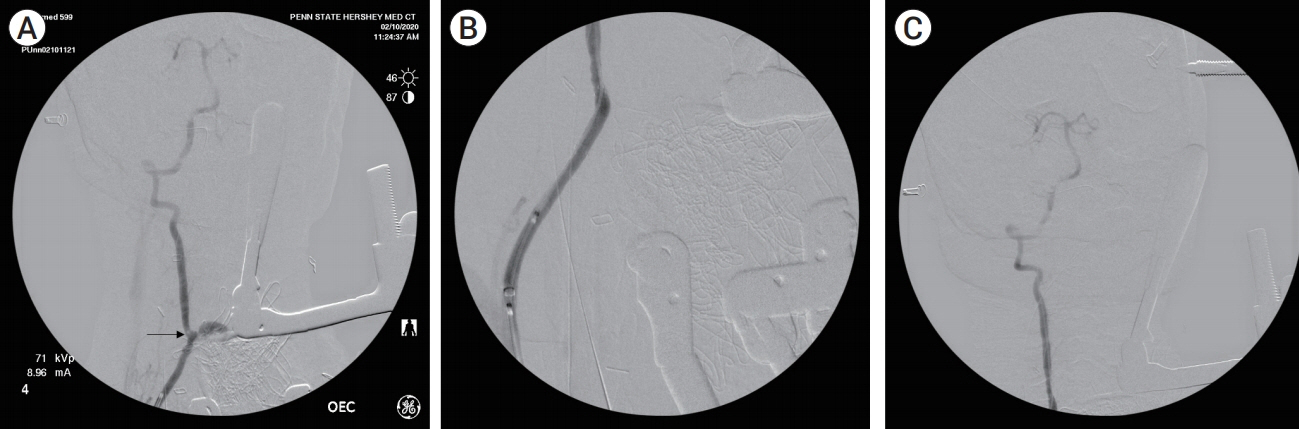
Fig. 2. Diagnostic angiogram following severe bleeding due to iatrogenic right-sided vertebral injury. Angiogram (A) demonstrates medial deviation of the right vertebral artery and a focal area of extravasation at C7 (arrow). (B) Angiogram demonstrat es placement of Viabahn covered stent. Angiogram (C) does not demonstrate opacification of suspected pseudoaneurysm, signaling obliteration.

Fig. 3. Post-operative cervical x-ray (A: AP view, B: lateral view) nine months post-operatively demonstrating correction of kyphosis, presence of bony fusion, and lack of hardware defects.
Reference
-
1. Bowry AD, Brookhart MA, Choudhry NK. Meta-analysis of the efficacy and safety of clopidogrel plus aspirin as compared to antiplatelet monotherapy for the prevention of vascular events. Am J Cardiol. 2008; Apr. 1. 101(7):960–6.
Article2. Carrillo-Martínez MÁ, Garza García GA, Leal Jacinto JM. Iatrogenic left vertebral artery pseudoaneurysm treated with a covered stent. BJR Case Rep. 2020; Sep. 29. 6(2):20190051.
Article3. Demetriades D, Theodorou D, Asensio J, Golshani S, Belzberg H, Yellin A, et al. Management options in vertebral artery injuries. Br J Surg. 1996; Jan. 83(1):83–6.
Article4. Geraghty PJ, Mewissen MW, Jaff MR, Ansel GM; VIBRANT Investigators. Three-year results of the VIBRANT trial of VIABAHN endoprosthesis versus bare nitinol stent implantation for complex superficial femoral artery occlusive disease. J Vasc Surg. 2013; Aug. 58(2):386–95.
Article5. Gurbel PA, Bliden KP, Butler K, Antonino MJ, Wei C, Teng R, et al. Response to ticagrelor in clopidogrel nonresponders and responders and effect of switching therapies: the RESPOND study. Circulation. 2010; Mar. 16. 121(10):1188–99.6. Safety and efficacy of ticagrelor for neuroendovascular procedures. A single center initial experience. J Neurointerv Surg. 2014; May. 6(4):320–2.7. Katsaridis V, Papagiannaki C, Violaris C. Treatment of an iatrogenic vertebral artery laceration with the Symbiot self expandable covered stent. Clin Neurol Neurosurg. 2007; Jul. 109(6):512–5.
Article8. Kim KS, Fraser JF, Grupke S, Cook AM. Management of antiplatelet therapy in patients undergoing neuroendovascular procedures. J Neurosurg. 2018; Oct. 129(4):890–905.
Article9. Lammer J, Zeller T, Hausegger KA, Schaefer PJ, Gschwendtner M, Mueller-Huelsbeck S, et al. Heparin-bonded covered stents versus bare-metal stents for complex femoropopliteal artery lesions: the randomized VIASTAR trial (Viabahn endoprosthesis with PROPATEN bioactive surface [VIA] versus bare nitinol stent in the treatment of long lesions in superficial femoral artery occlusive disease). J Am Coll Cardiol. 2013; Oct. 8. 62(15):1320–7.10. Meier DE, Brink BE, Fry WJ. Vertebral artery trauma: acute recognition and treatment. Arch Surg. 1981; Feb. 116(2):236–9.11. Saxon RR, Chervu A, Jones PA, Bajwa TK, Gable DR, Soukas PA, et al. Heparin-bonded, expanded polytetrafluoroethylene-lined stent graft in the treatment of femoropopliteal artery disease: 1-year results of the VIPER (Viabahn Endoprosthesis with Heparin Bioactive Surface in the Treatment of Superficial Femoral Artery Obstructive Disease) trial. J Vasc Interv Radiol. 2013; Feb. 24(2):165–73. quiz 174.
Article12. Stain SC, Yellin AE, Weaver FA, Pentecost MJ. Selective management of nonocclusive arterial injuries. Arch Surg. 1989; Oct. 124(10):1136–40. discussion 1140.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Management of Iatrogenic Vertebral Artery Pseudoaneurysm: A Case Report
- Jejunal Migration of the Stent-Graft Used for Common Hepatic Artery Pseudoaneurysm
- Epidemiology and Management of Iatrogenic Vertebral Artery Injury Associated With Cervical Spine Surgery
- Endovascular Stent-Graft Treatment of a Traumatic Vertebral Artery Pseudoaneurysm and Vertebrojugular Fistula
- Iatrogenic Vertebral Artery Injury During Anterior Cervical Spine Surgery : Report of Two Cases
