Congenital Long QT Syndrome Type 2 with Symptomatic 2:1 Atrioventricular Block and Ventricular Arrhythmia in a Preterm Baby Who Presented with Fetal Ventricular Tachycardia and Hydrops
- Affiliations
-
- 1Department of Pediatrics, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 2Department of Pediatrics, Incheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2519842
- DOI: http://doi.org/10.4070/kcj.2021.0202
Figure
-
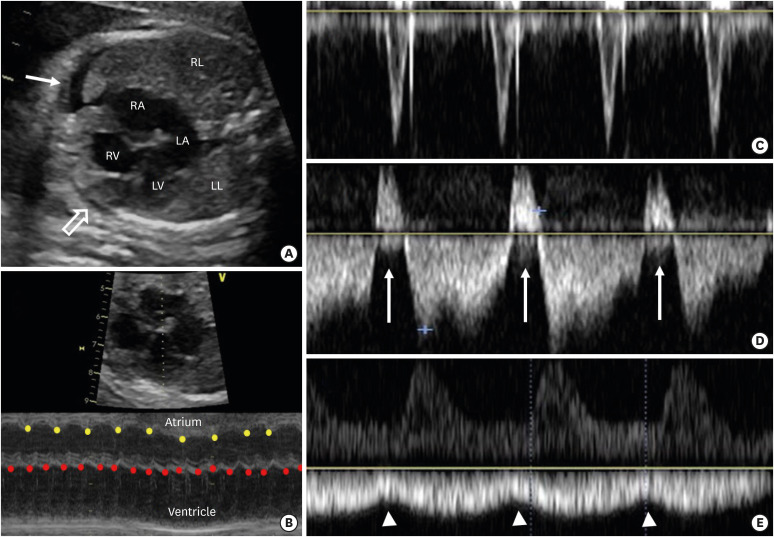
Figure 1 Fetal echocardiography images. (A) A transverse scanning with a four-chamber view shows enlarged right atrium, dilated and hypertrophied right ventricle, small amount of pericardial effusion (open arrow), and pleural effusion (closed arrow). (B) An M-mode image shows a ventricular tachycardia (red dots) with a heart rate of 215 beats/min, instead atrial rate (yellow dots) is 120 beats/min. (C) Tricuspid valve inflow Doppler shows a sharp monophasic filling pattern. (D) A ductus venosus flow Doppler shows reverse flows during atrial contractions (arrows). (E) An umbilical venous flow Doppler shows notches during atrial contractions (arrow heads). All of the above findings suggest severe fetal cardiovascular dysfunction and poor general conditions, which demand immediate treatment.1) Image C, D and E were obtained during the time without ventricular tachycardia.LA = left atrium; LL = left lung; LV = left ventricle; RA = right atrium; RL = right lung; RV = right ventricle.
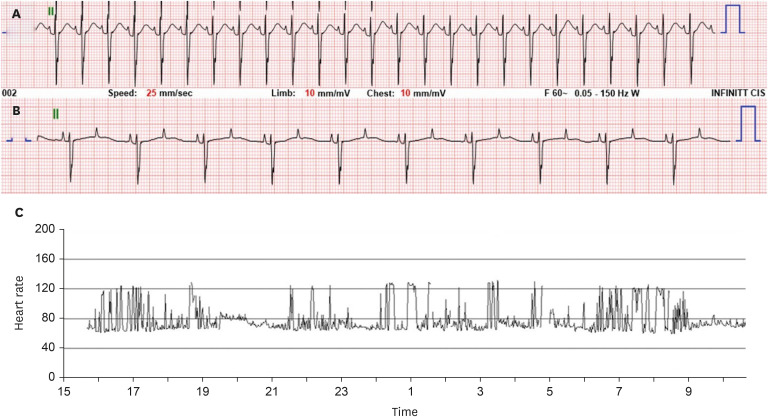
Figure 2 Electrocardiograms after birth showing a sinus rhythm with a heart rate of 166 beats/min and prolonged QT interval (QTc = 530 ms) (A) and frequent 2:1 atrioventricular blocks with a heart rate of 50–60 beats/min (B). Severe sudden heart rate fluctuations (50–130 beats/min) were observed on Holter monitoring (C).
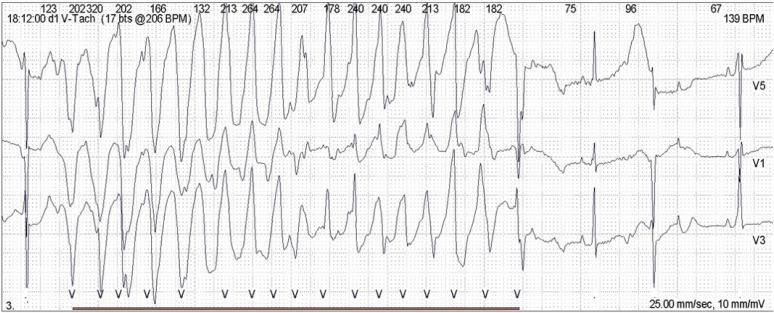
Figure 3 Electrocardiogram at 1 month of age, showing a polymorphic ventricular tachycardia (Torsades de pointes), which occurred 2–3 times a day.
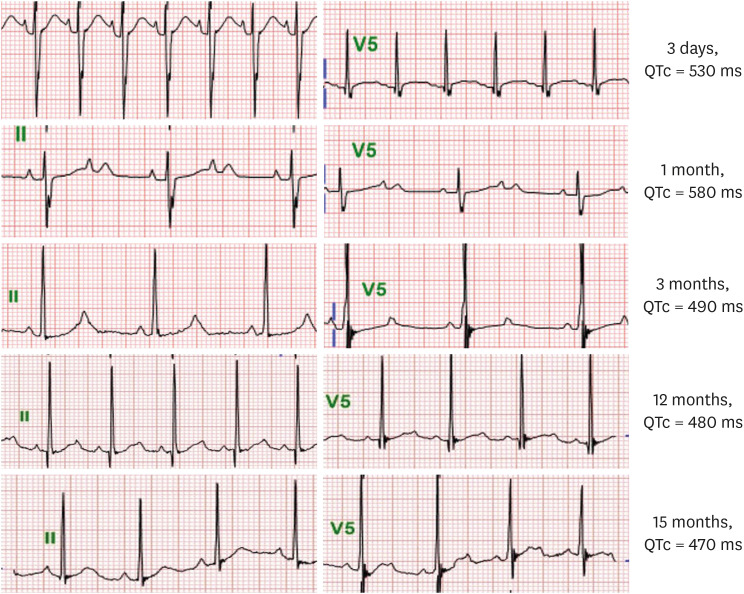
Figure 4 Serial changes of electrocardiogram (lead II and V5) and corrected QT intervals (QTc) over time according to the age of the patient. Electrocardiograms at 1 and 3 months of age showed 2:1 atrioventricular blocks and thereafter, normal sinus rhythms.
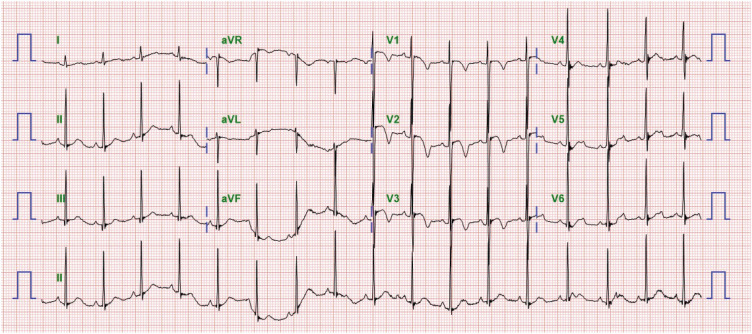
Figure 5 Electrocardiogram at 15 months of age showing a sinus rhythm with a QTc of 470 ms, and notched and asymmetrical T-waves, which are rather typical T-wave morphology in LQT2.
Reference
-
1. Li Y, Fang J, Zhou K, et al. Prediction of fetal outcome without intrauterine intervention using a cardiovascular profile score: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2015; 28:1965–1972. PMID: 25308207.
Article2. Miyake A, Sakaguchi H, Miyazaki A, Miyoshi T, Aiba T, Shiraishi I. Successful prenatal management of ventricular tachycardia and second-degree atrioventricular block in fetal long QT syndrome. HeartRhythm Case Rep. 2016; 3:53–57. PMID: 28491768.
Article3. Aziz PF, Tanel RE, Zelster IJ, et al. Congenital long QT syndrome and 2:1 atrioventricular block: an optimistic outcome in the current era. Heart Rhythm. 2010; 7:781–785. PMID: 20197117.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Congenital Long OT Syndrome with Pseudo - Atrioventricular Block
- Two Cases of 2:1 Atrioventricular Block in Infants with Idiopathic Long QT Syndrome
- A Case of Congenital Long QT Syndrome Associated with Deafness and Syncope
- Left Stellate Ganglion Block Prior to Induction of Anesthesia for Surgical Sympathectomy in a Patient with Long QT Syndrome
- Congenital Long QT Syndrome Type 8 Characterized by Fetal Onset of Bradycardia and 2:1 Atrioventricular Block
