A Case of Free Flap Reconstruction after Endoscopic Debridemnt for Recalcitrant Nasopharyngeal Osteoradionecrosis Without Facial Incision
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2518679
- DOI: http://doi.org/10.18787/jr.2021.00353
Abstract
- High-dose radiation therapy is the treatment of choice for nasopharyngeal cancer, and clinical outcomes have improved in recent decades. A certain proportion of patients, however, suffer from post-radiation nasopharyngeal necrosis (PRNN). Patients with PRNN complain of headache, foul odor, or symptoms of cranial nerve palsies. Clinically, intracranial infection or bleeding from carotid artery damage may lead to sudden death or severe deterioration in quality of life. Although the prognosis of PRNN was poor, endoscopic debridement with local vascularized flap recently showed favorable outcomes, and many centers are using this technique with a nasoseptal flap. However, if the flap fails or does not fully cover necrotized tissues, necrosis inevitably reoccurs. In this situation, free flap transfer with a facial incision using a transmaxillary approach is used, but some drawbacks exist. In this report, we propose a new resurfacing technique for recurrent PRNN using a transoral-cervical free flap tunneling approach into the nasopharynx without a facial incision after endoscopic debridement.
Keyword
Figure
-

Fig. 1. Endoscopic, radiologic, intraoperative image of nasopharynx radionecrosis. A: Transnasal endoscopic view showed mucosal necrosis on right nasopharynx. B: T1 Gadolinium enhanced MRI showed irregular enhancement and non-enhancing lesion around the right lateral and posterior wall of nasopharynx (black arrow). C: Intraoperative endoscopic view after endoscopic debridement. Remained muscle looks relatively healthy.
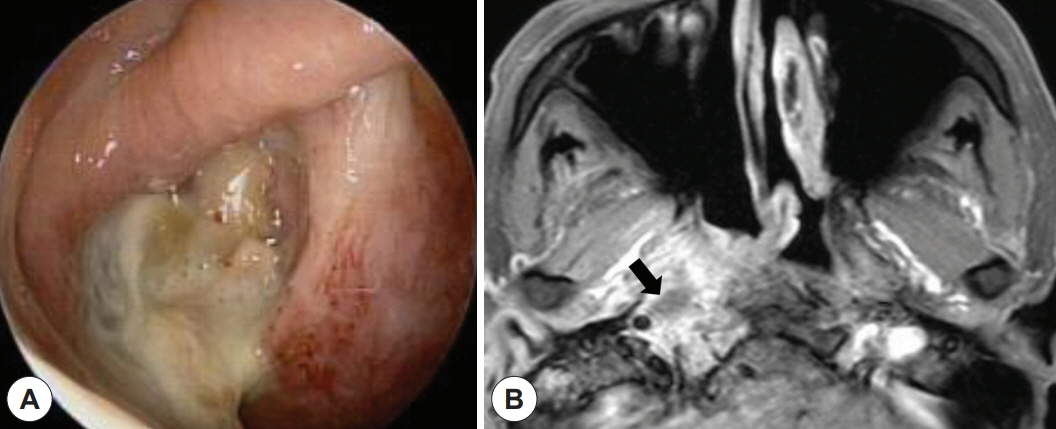
Fig. 2. Endoscopic, radiologic image of recurrent nasopharynx radionecrosis. A: Recurrent necrosis inferior to well adapted nasoseptal flap. B: T1 Gadolinium enhanced MRI showed nonenhanced area (necrosis) surrounded by enhanced muscle (black arrow).

Fig. 3. Postoperative endoscopic and radiologic image of flap wound, surgical schematic diagram. A: Postop 2 weeks transoral view. Arrow indicates flap. B: Postop 2 weeks transnasal view. Arrow indicates flap. C: Postop 4 months transoral view. Arrow indicates flap. D: Postop 4 months transnasal view. Arrow indicates flap. E: Postop 14 months transoral view. Arrow indicates flap. F: Postop 14 months transnasal view. Arrow indicates flap. G: Postop 14 months T1 Gadolinium enhanced MRI showed well enhanced NSF and well positioned free flap (white arrow). H: Surgical Schematic diagram of transoral approach anterolateral thigh free flap into nasopharynx without facial incision.
Reference
-
References
1. Lee HM, Okuda KS, González FE, Patel V. Current perspectives on nasopharyngeal carcinoma. In : Rhim JS, Dritschilo A, Kremer R, editors. Human Cell Transformation. Cham, Switzerland: Springer;2019. p. 11–34.2. Han P, Wang X, Liang F, Liu Y, Qiu X, Xu Y, et al. Osteoradionecrosis of the Skull Base in Nasopharyngeal Carcinoma: Incidence and Risk Factors. Int J Radiat Oncol Biol Phys. 2018; 102(3):552–5.3. Marx RE. Osteoradionecrosis: a new concept of its pathophysiology. J Oral Millofac Surg. 1983; 41(5):283–8.4. Huang XM, Zheng YQ, Zhang XM, Mai HQ, Zeng L, Liu X, et al. Diagnosis and management of skull base osteoradionecrosis after radiotherapy for nasopharyngeal carcinoma. Laryngoscope. 2006; 116(9):1626–31.5. Cho SW, Won TB. Management of Skull Base Osteoradionecrosis. Korean J Otorhinolaryngol-Head Neck Surg. 2020; 63(2):51–8.6. Huang WB, Wong STS, Chan JYW. Role of surgery in the treatment of osteoradionecrosis and its complications after radiotherapy for nasopharyngeal carcinoma. Head Neck. 2018; 40(2):369–76.7. Chang KP, Tsang NM, Chen CY, Su JL, Hao SP. Endoscopic management of skull base osteoradionecrosis. Laryngoscope. 2000; 110(7):1162–5.8. Choi NY, Kim HJ, Baek CH. Surgical management of extensive osteoradionecrosis in nasopharyngeal carcinoma patients with the maxillary swing approach and free muscular flaps. Clin Otolaryngol. 2017; 42(5):1100–4.9. Lan G, Huang B, Si Y, Qin Y, Deng Z, Yang Y, et al. [The clinical experience of transnasal endoscopic approach for skull base osteoradionecrosis after radiotherapy for nasopharyngeal carcinoma]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2016; 51(5):367–71.10. Liu J, Ning X, Sun X, Lu H, Gu Y, Wang D. Endoscopic sequestrectomy for skull base osteoradionecrosis in nasopharyngeal carcinoma patients: a 10year experience. Int J Clin Oncol. 2019; 24(3):248–55.11. Adel M, Chang KP. Using a nasoseptal flap for the reconstruction of osteoradionecrosis in nasopharyngeal carcinoma: a case report. J Otolaryngol Head Neck Surg. 2016; 45(1):27.12. Ryu G, So YK, Seo MY, Park W, Kim HY, Dhong HJ, et al. Using the nasoseptal flap for reconstruction after endoscopic debridement of radionecrosis in nasopharyngeal carcinoma. Am J Rhinol Allergy. 2018; 32(1):61–5.13. Yang Q, Zou X, You R, Liu YP, Han Y, Zhang YN, et al. Proposal for a new risk classification system for nasopharyngeal carcinoma patients with post-radiation nasopharyngeal necrosis. Oral Oncol. 2017; 67:83–8.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Buccinator Myomucosal Flap for Treatment of Osteoradionecrosis of the Mandible
- Reconstruction with fibular osteocutaneous free flap in patients with mandibular osteoradionecrosis
- Reconstruction using fibular osteocutaneous free flap of squamous cell carcinoma occurred in mandibular alveolar ridge accompanied with osteoradionecrosis
- Treatment of chest wall osteoradionecrosis with a contralateral breast Y-V flap: a case report
- Various Flap for Treatment of Radiation Ulcer and Osteoradionecrosis
