Microcatheter Stabilization Technique Using Partially Inflated Balloon for Coil Embolization of Paraclinoid Aneurysms
- Affiliations
-
- 1Neurointervention Clinic, Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Diagnostic and Interventional Radiology Department, Imam Abdulrahman Bin Faisal University, King Fahd Hospital of the University, Al-Khobar City, Saudi Arabia
- 3Neurovascular Division National Brain Center Prof. Dr. Mahar Mardjono Hospital, Jakarta, Indonesia
- KMID: 2517738
- DOI: http://doi.org/10.5469/neuroint.2021.00185
Abstract
- Purpose
Coil embolization of paraclinoid aneurysms should be simple, safe, and effective considering the benign nature of the aneurysm. Here, we present a microcatheter stabilization technique using a partially inflated balloon for the treatment of paraclinoid aneurysms.
Materials and Methods
This retrospective study included 58 patients who underwent balloon-assisted coiling (BAC) for unruptured paraclinoid aneurysms at a tertiary neuro-intervention center between January 2019 and March 2020. We applied a technique to stabilize the microcatheter’s position using the modified BAC technique in paraclinoid aneurysms showing various projections around the ophthalmic curve of the internal carotid artery. The basic concept of the technique is to place a partially inflated balloon just distal to the aneurysm neck and support the distal curve of the microcatheter using the proximal bottom of the balloon. Immediate radiological outcomes were analyzed, and clinical outcomes were evaluated with modified Rankin Scale (mRS) scores.
Results
The BAC was successfully performed in 51 of 58 patients (88%). We treated the remaining seven patients by switching to stent-assisted coiling. We obtained a 37% mean packing density resulting in favorable occlusion in all 58 aneurysms (complete occlusion in 35 and residual neck in 23). There were no intraprocedural thromboembolic or hemorrhagic events except one that revealed an asymptomatic infarction after the procedure (1.7%). Magnetic resonance angiography follow-up was performed in 37 patients at an average of 11.8 months, in which 11 minor recurrences (29.7%) were found. There was no major recurrence nor retreatment. The mRS score was 0 in all patients during a mean follow-up of 17.7 months (range, 12–25 months).
Conclusion
The modified balloon-assisted coiling technique using a partially inflated balloon was safe and effective and could serve as an option for treating paraclinoid aneurysms.
Figure
-
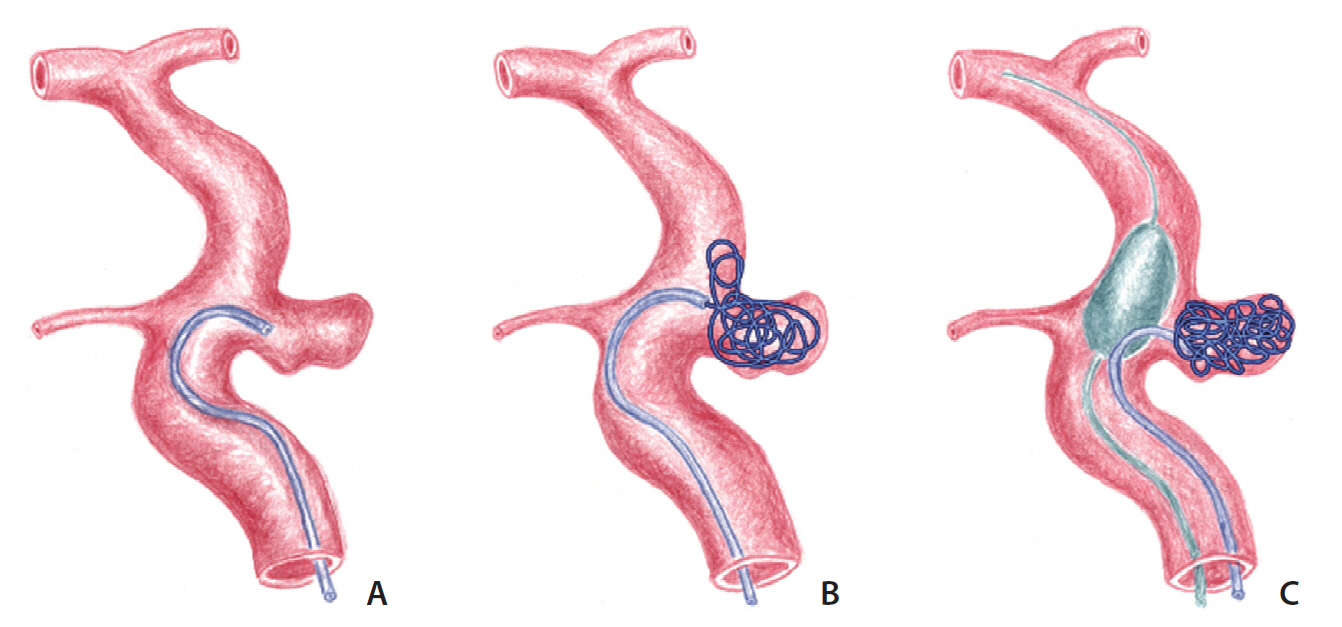
Fig. 1. Concept diagram depicting coiling of the paraclinoid aneurysm using a partially inflated balloon. (A) A loop-shaped microcatheter is introduced into the aneurysm. (B) The coil protrudes out of the aneurysm because of resistance of the coil within the aneurysm and withdrawal of the microcatheter. (C) Coil packing can be accomplished by supporting the microcatheter loop with the partially inflated balloon.
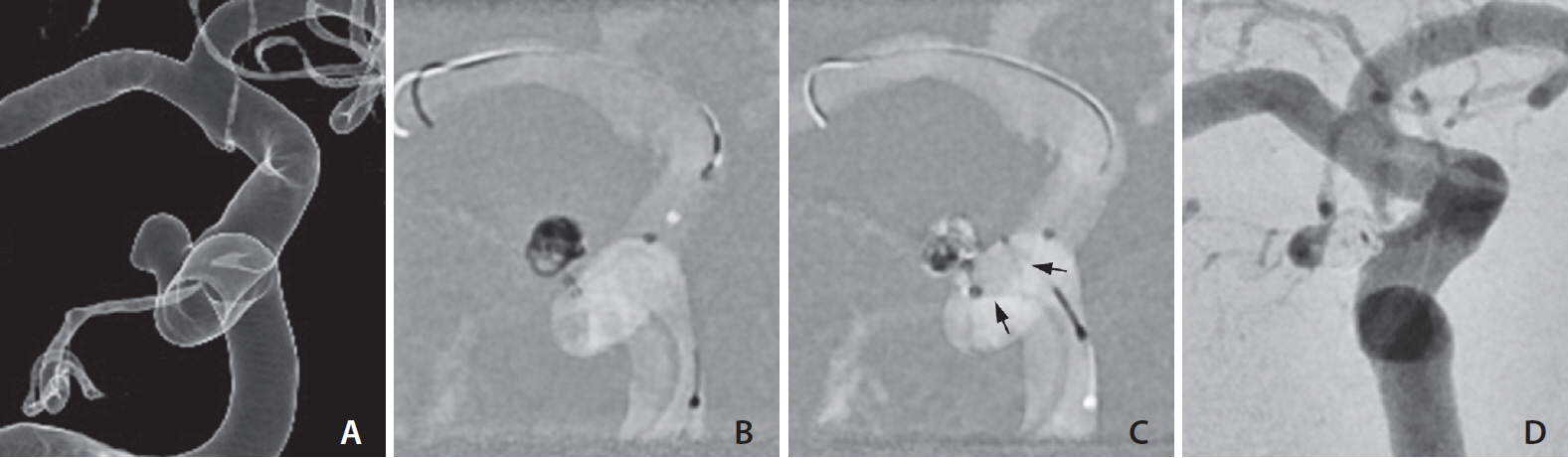
Fig. 2. Balloon-assisted coiling for the treatment of a paraclinoid aneurysm. (A) A 4-mm aneurysm with superolateral projection just distal to the anterior genus of the right cavernous internal carotid artery. (B, C) Framing and filling coils are inserted into the aneurysm by supporting the microcatheter with intermittent ballooning (arrows). (D) No contrast filling is seen in the aneurysm on completion angiogram. A tiny opacification within the coil mass was determined as an overlapping ophthalmic artery.
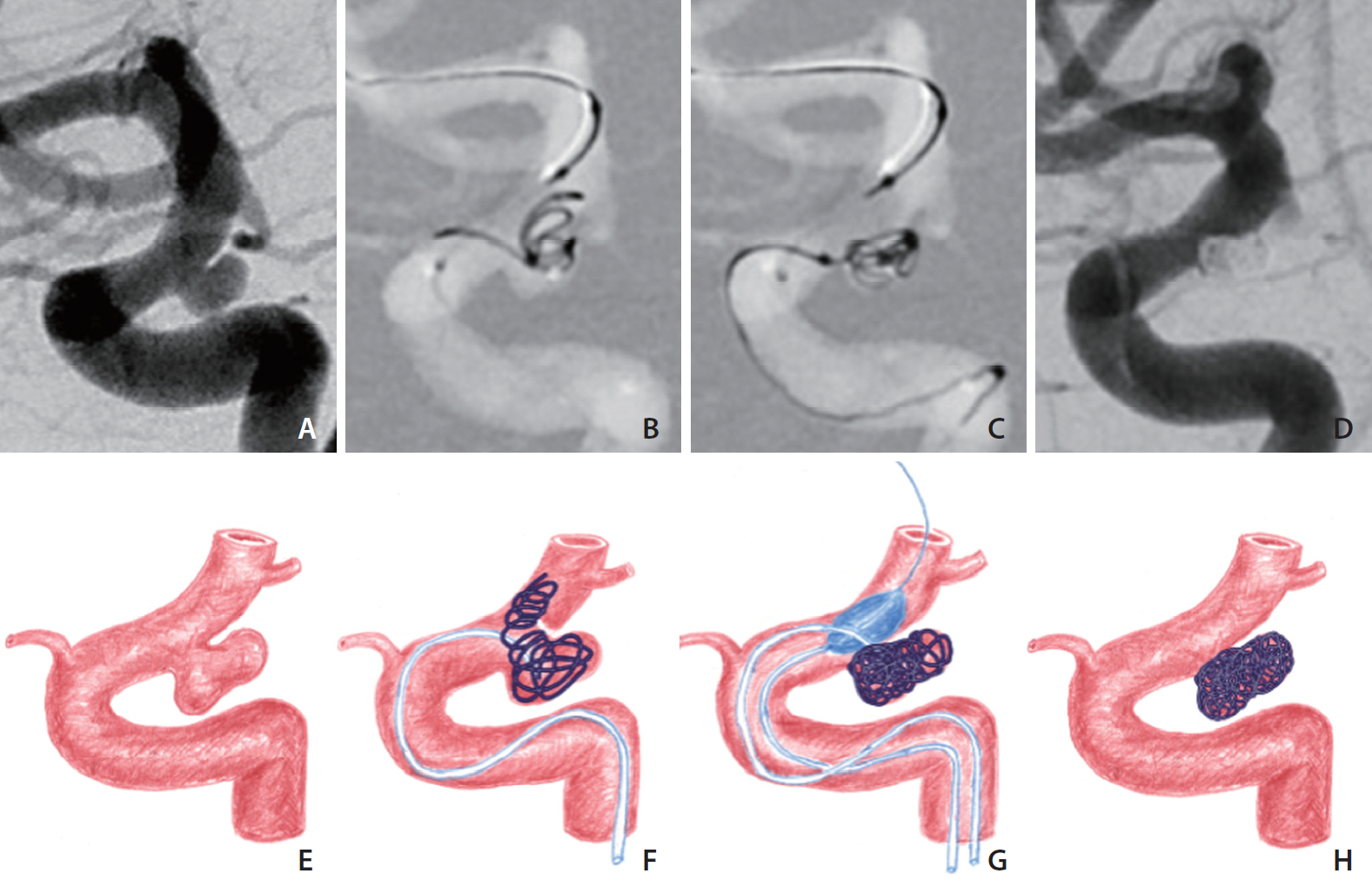
Fig. 3. A paraclinoid aneurysm with a relatively well-delineated neck as a pseudo-neck. (A) An internal carotid arteriogram shows an aneurysm at the posterior wall. (B) The aneurysm neck is not resistant to the coils and collapses while introducing the frame coil; thus it is regarded as a pseudo-neck. (C) The coils are contained within the aneurysm via the balloon inflation. (D) Final angiogram shows compact coiling of the aneurysm. (E–H) Concept diagrams of the procedure.
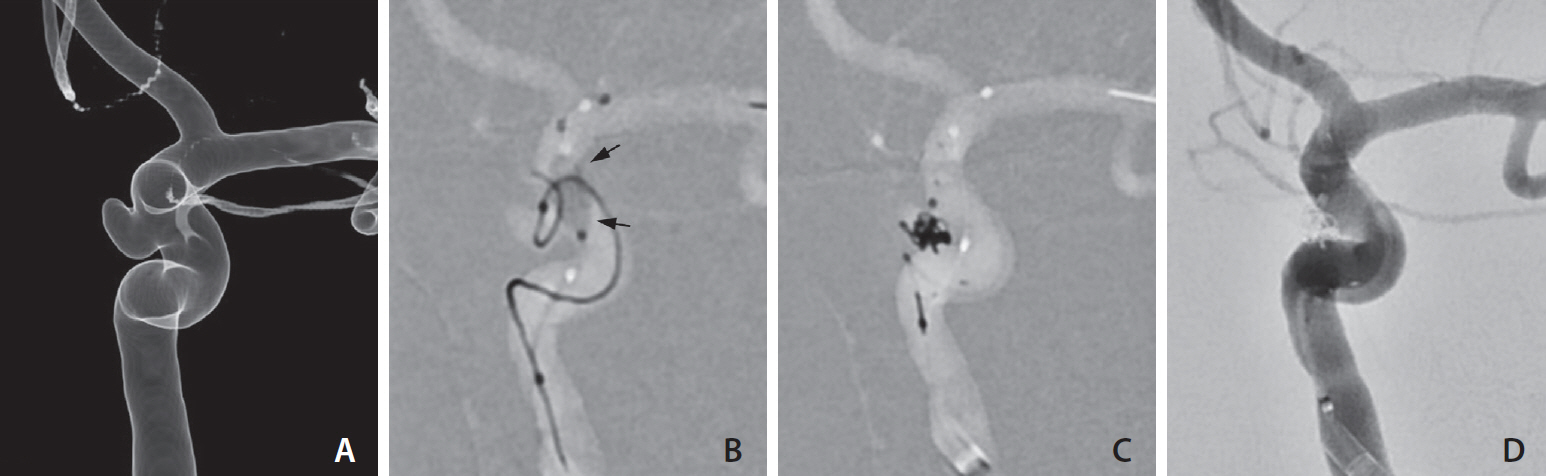
Fig. 4. Exchange into stenting after the failure of balloon-assisted coiling. (A) Left internal carotid angiogram shows an aneurysm projecting medially. (B) Despite using a balloon (arrows), the coil protrudes out of the aneurysm. (C) After deploying a stent, the coil is packed in the aneurysm. (D) Complete obliteration of the aneurysm is achieved.
Reference
-
1. Kwon BJ, Im SH, Park JC, Cho YD, Kang HS, Kim JE, et al. Shaping and navigating methods of microcatheters for endovascular treatment of paraclinoid aneurysms. Neurosurgery. 2010; 67:34–40. discussion 40.
Article2. Bouthillier A, van Loveren HR, Keller JT. Segments of the internal carotid artery: a new classification. Neurosurgery. 1996; 38:425–432. discussion 432-433.
Article3. D’Urso PI, Karadeli HH, Kallmes DF, Cloft HJ, Lanzino G. Coiling for paraclinoid aneurysms: time to make way for flow diverters? AJNR Am J Neuroradiol. 2012; 33:1470–1474.
Article4. Wang Y, Li Y, Jiang C, Jiang F, Meng H, Siddiqui AH, et al. Endovascular treatment of paraclinoid aneurysms: 142 aneurysms in one centre. J Neurointerv Surg. 2013; 5:552–556.
Article5. Kwon WH, Jeong HW, Kim ST, Seo JH. Angiographic and clinical result of endovascular treatment in paraclinoid aneurysms. Neurointervention. 2014; 9:83–88.
Article6. Suh SH. The annual trends between neurointerventional and neurosurgical procedures in Korea: analysis using HIRA data from 2010 to 2016. Neurointervention. 2017; 12:77–82.
Article7. Sun Y, Li Y, Li AM. Endovascular treatment of paraclinoid aneurysms. Interv Neuroradiol. 2011; 17:425–430.
Article8. Cho YD, Rhim JK, Park JJ, Jeon JS, Yoo RE, Kang HS, et al. Microcatheter looping to facilitate aneurysm selection in coil embolization of paraclinoid aneurysms. Korean J Radiol. 2015; 16:899–905.
Article9. Sheen JJ, Suh DC. Low-angled microcatheter approach for coil embolization of the anterior choroidal artery aneurysm. Neuroradiology. 2017; 59:1053–1056.
Article10. Nelson PK, Levy DI. Balloon-assisted coil embolization of widenecked aneurysms of the internal carotid artery: medium-term angiographic and clinical follow-up in 22 patients. AJNR Am J Neuroradiol. 2001; 22:19–26.11. Santillan A, Gobin YP, Mazura JC, Meausoone V, Leng LZ, Greenberg E, et al. Balloon-assisted coil embolization of intracranial aneurysms is not associated with increased periprocedural complications. J Neurointerv Surg. 2013; 5 Suppl 3:iii56–iii61.
Article12. Pop R, Harsan O, Martin I, Mihoc D, Richter JS, Manisor M, et al. Balloon-assisted coiling of intracranial aneurysms using the Eclipse 2L double lumen balloon. Interv Neuroradiol. 2020; 26:291–299.
Article13. Wallace AN, Samaniego E, Kayan Y, Derdeyn CP, Delgado Almandoz JE, Dandapat S, et al. Balloon-assisted coiling of cerebral aneurysms with the dual-lumen Scepter XC balloon catheter: experience at two high-volume centers. Interv Neuroradiol. 2019; 25:414–418.
Article14. Spiotta AM, Miranpuri A, Hawk H, Chaudry MI, Turk AS, Turner RD. Balloon remodeling for aneurysm coil embolization with the coaxial lumen Scepter C balloon catheter: initial experience at a high volume center. J Neurointerv Surg. 2013; 5:582–585.
Article15. Sluzewski M, van Rooij WJ, Beute GN, Nijssen PC. Balloon-assisted coil embolization of intracranial aneurysms: incidence, complications, and angiography results. J Neurosurg. 2006; 105:396–399.
Article16. Shapiro M, Babb J, Becske T, Nelson PK. Safety and efficacy of adjunctive balloon remodeling during endovascular treatment of intracranial aneurysms: a literature review. AJNR Am J Neuroradiol. 2008; 29:1777–1781.
Article17. Pierot L, Spelle L, Leclerc X, Cognard C, Bonafé A, Moret J. Endovascular treatment of unruptured intracranial aneurysms: comparison of safety of remodeling technique and standard treatment with coils. Radiology. 2009; 251:846–855.
Article18. Pierot L, Cognard C, Anxionnat R, Ricolfi F; CLARITY Investigators. Remodeling technique for endovascular treatment of ruptured intracranial aneurysms had a higher rate of adequate postoperative occlusion than did conventional coil embolization with comparable safety. Radiology. 2011; 258:546–553.
Article19. Jia ZY, Shi HB, Miyachi S, Hwang SM, Sheen JJ, Song YS, et al. Development of new endovascular devices for aneurysm treatment. J Stroke. 2018; 20:46–56.
Article20. Kim JJ, Cho KC, Jung WS, Suh SH. Endovascular treatment for intracranial aneurysms: a nationwide survey in Korea. Neurointervention. 2020; 15:18–24.
Article21. Shapiro M, Becske T, Riina HA, Raz E, Zumofen D, Jafar JJ, et al. Toward an endovascular internal carotid artery classification system. AJNR Am J Neuroradiol. 2014; 35:230–236.
Article22. Brinjikji W, Cloft HJ, Kallmes DF. Difficult aneurysms for endovascular treatment: overwide or undertall? AJNR Am J Neuroradiol. 2009; 30:1513–1517.
Article23. Lee D, Song Y, Shin JH, Suh DC. Low-dose prasugrel in patients with resistance to clopidogrel for the treatment of cerebral aneurysms: follow-up of over 6 months. Neurointervention. 2019; 14:68–70.
Article24. Lee D, Song Y, Han M, Park D, Suh DC. Low-dose prasugrel in patients with resistance to clopidogrel for the treatment of cerebral aneurysms. Neurointervention. 2018; 13:124–127.
Article25. Kurniawan RG, Song Y, Kwon B, Ahn Y, Suh DC. Tailored antiplatelet agent medication in clopidogrel hyporesponsive patients before stent-assisted coiling: single-center experience. Neuroradiology. 2020; 62:1709–1715.
Article26. Jia ZY, Song YS, Sheen JJ, Kim JG, Lee CW, Suh DC. Loop microcatheter technique for coil embolization of paraclinoid aneurysms. Acta Neurochir (Wien). 2018; 160:1755–1760.
Article27. Kim DY, Park JC, Kim JK, Sung YS, Park ES, Kwak JH, et al. Microembolism after endovascular treatment of unruptured cerebral aneurysms: reduction of its incidence by microcatheter lumen aspiration. Neurointervention. 2015; 10:67–73.
Article28. Cho YD, Kim KM, Lee WJ, Sohn CH, Kang HS, Kim JE, et al. Time-of-flight magnetic resonance angiography for follow-up of coil embolization with enterprise stent for intracranial aneurysm: usefulness of source images. Korean J Radiol. 2014; 15:161–168.
Article29. Roy D, Milot G, Raymond J. Endovascular treatment of unruptured aneurysms. Stroke. 2001; 32:1998–2004.
Article30. Raymond J, Guilbert F, Weill A, Georganos SA, Juravsky L, Lambert A, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke. 2003; 34:1398–1403.
Article31. Yamaguchi S, Ito O, Koyanagi Y, Iwaki K, Matsukado K. Microcatheter shaping using intravascular placement during intracranial aneurysm coiling. Interv Neuroradiol. 2017; 23:249–254.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Microcatheter Looping to Facilitate Aneurysm Selection in Coil Embolization of Paraclinoid Aneurysms
- Parent Artery Complex Coil Protection for Side-Branched Wide-Neck Aneurysms
- Aneurysm Coil Embolization Using a 1.5-Fr Distal Outer Diameter Microcatheter
- Microcatheter-assisted Coil Embolization of Distal Vertebral Artery Wide-Necked Aneurysm: A Case Report
- Endovascular Rescue Method for Undesirably Stretched Coil
