Hepatic artery aneurysms: Endovascular therapeutic techniques
- Affiliations
-
- 1Department of Radiological Area, Interventional Radiology Unit, E.O. Galliera Hospital, Genova, Italy
- 2Department of Radiology and Interventional Radiology, IRCCS San Martino Policlinic University Hospital, Genova, Italy
- KMID: 2516236
- DOI: http://doi.org/10.14701/ahbps.2021.25.2.167
Abstract
- Hepatic Artery Aneurysm (HAA) is a rare disease, but it can be a life-threatening pathology if it is ruptured. MultiDetector Computed Tomography has to be considered the “gold standard” diagnostic imaging in detecting HAA and it is essential for treatment planning. Treatment for HAA can be surgical or endovascular. Endovascular approaches in HAA, compare to conventional abdominal surgery, benefit in less invasive treatments. The aim of our paper is to emphasize the three possible endovascular therapeutic techniques in HAA: packing embolization, isolation embolization and stenting deployment.
Keyword
Figure
-
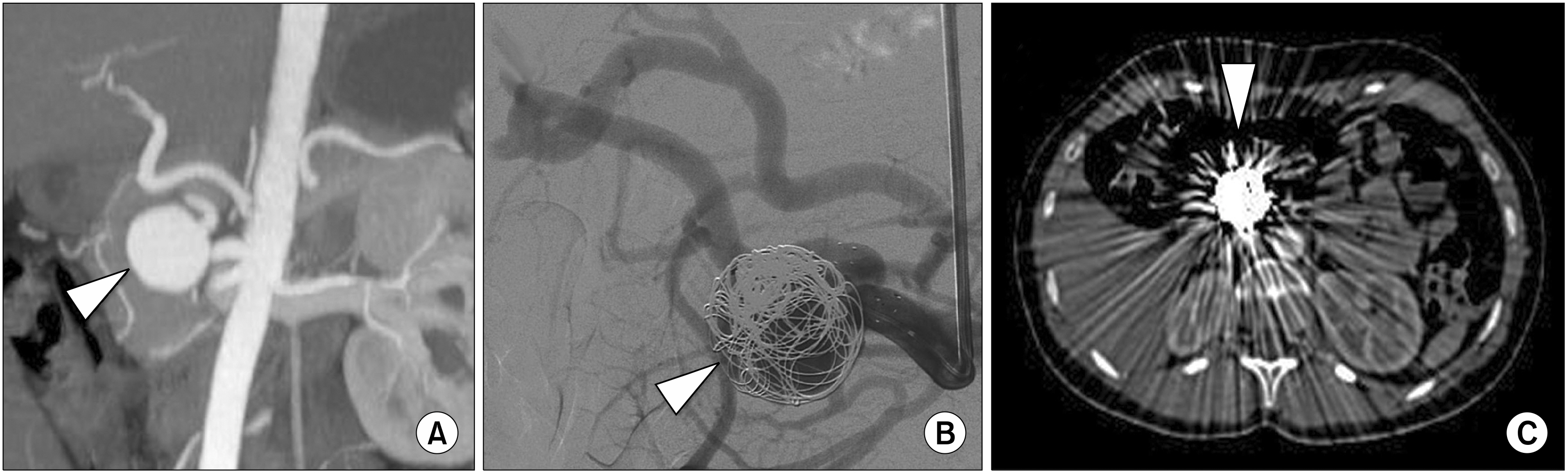
Fig. 1 (A) Contrast enhanced Multi-Detector Computed Tomography coronal MIP reconstruction image of the upper abdomen that shows a saccular right hepatic artery aneurysm of 3 cm in diameter (arrowhead). (B) Selective right hepatic artery Digital Subtraction Angiography during coil devices deployment into the aneurysm sac (arrowhead). (C) Contrast enhanced Multi-Detector Computed Tomography axial image at 6-months follow-up that confirms the presence of coils into the right hepatic artery aneurism (arrowhead) with multiple metallic artefact.

Fig. 2 (A) Contrast enhanced Multi-Detector Computed Tomography coronal MIP reconstruction image of the upper abdomen that shows a hepatic artery fusiform aneurysm of 3.7 cm in diameter (arrowhead), a focal wall tear with contrast media extravasation as sign of rupture (arrow) and dilatation of the right and left hepatic arteries. (B) Selective hepatic artery Digital Subtraction Angiography that confirms the hepatic artery fusiform aneurysm (arrowhead) and the focal wall tear with contrast media extravasation as sign of rupture (arrow). (C) Final selective hepatic artery Digital Subtraction Angiography that confirms the exclusion of hepatic artery fusiform aneurysm with isolation embolization technique by coils deployment into right and left hepatic arteries (arrows) and into post-origin of common hepatica artery (arrowhead). (D) Contrast enhanced Multi-Detector Computed Tomography coronal MPR reconstruction image of the upper abdomen at 12-months follow-up that confirms the exclusion of hepatic artery fusiform aneurysm with coils artefacts at the level of right and left hepatic arteries (arrows) and post-origin of common hepatica artery (arrowhead).
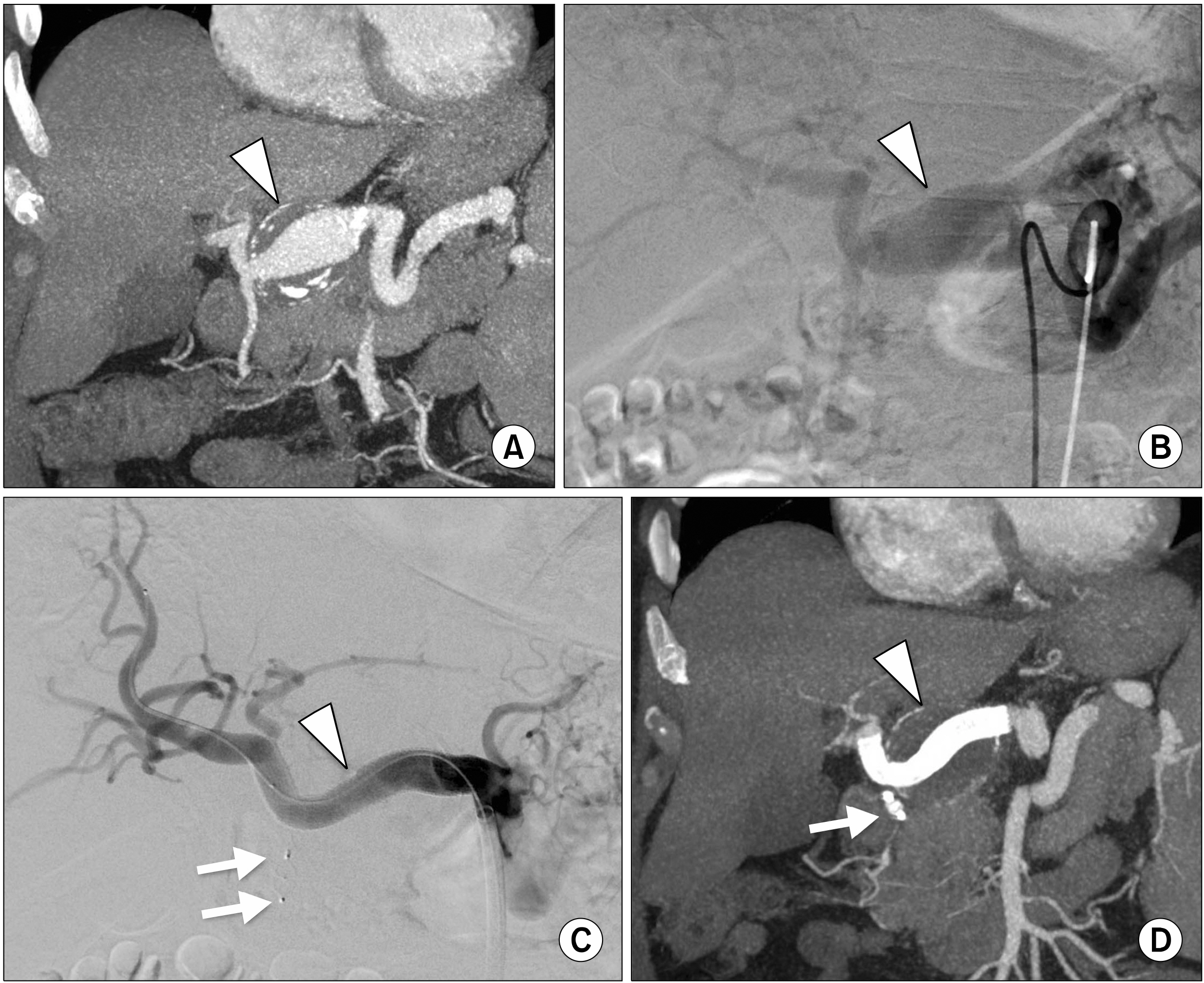
Fig. 3 (A) Contrast enhanced Multi-Detector Computed Tomography coronal MIP reconstruction image of the upper abdomen that shows a common hepatic artery aneurysm of 3.8 cm in diameter with partial thrombosis and wall calcifications (arrowhead), (B) Selective hepatic artery Digital Subtraction Angiography that confirms common hepatic artery aneurysm (arrowhead). (C) Final selective hepatic artery Digital Subtraction Angiography that confirms the exclusion of common hepatic artery aneurysm by covered stent deployment (arrowhead) with distal artery patency; note the two metal artefact of plug device deployed at the origin of gastroduodenal artery (arrows). (D) Contrast enhanced Multi-Detector Computed Tomography coronal MPR reconstruction image of the upper abdomen at 24-months follow-up that confirms the exclusion common hepatic artery aneurysm by covered stent deployment (arrowhead) and metal artefact at gastroduodenal artery origin due to plug device (arrow).
Reference
-
1. Rosenberg A, Trebska-McGowan K, Reichman T, Sharma A, Cotterell A, Strife B, et al. 2020; Management of hepatic artery aneurysm: a case series. Ann Hepatobiliary Pancreat Surg. 24:333–338. DOI: 10.14701/ahbps.2020.24.3.333. PMID: 32843601. PMCID: PMC7452805.
Article2. Obara H, Kentaro M, Inoue M, Kitagawa Y. 2020; Current management strategies for visceral artery aneurysms: an overview. Surg Today. 50:38–49. DOI: 10.1007/s00595-019-01898-3. PMID: 31620866. PMCID: PMC6949316.
Article3. Chiaradia M, Novelli L, Deux JF, Tacher V, Mayer J, You K, et al. 2015; Ruptured visceral artery aneurysms. Diagn Interv Imaging. 96:797–806. DOI: 10.1016/j.diii.2015.03.012. PMID: 26054246.
Article4. Ferro C, Rossi UG, Bovio G, Petrocelli F, Seitun S. 2010; The Amplatzer vascular plug 4: preliminary experience. Cardiovasc Intervent Radiol. 33:844–848. DOI: 10.1007/s00270-009-9749-6. PMID: 19908084.
Article5. Ferro C, Rossi UG, Seitun S, Bovio G, Castellan L, De Paolis M, et al. 2008; Hepatic arterial loop with accessory right hepatic artery aneurysm with celiac atresia: endovascular therapy with a stent and detachable coils. J Vasc Interv Radiol. 19:1236–1240. DOI: 10.1016/j.jvir.2008.05.005. PMID: 18656020.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Right Gastroepiploic Artery Transposition for a Common Hepatic Artery and Proper Hepatic Artery Aneurysm Repair
- Endovascular Management of Hepatic Artery Pseudoaneurysms: A Case Series
- Endovascular Treatment of Multiple Pancreaticoduodenal Artery Aneurysms Associated with Celiac Artery Stenosis: A Case Report
- Kissing Aneurysms at Fenestrated Proximal Basilar Artery: Double-barrel Stent-assisted Coiling Using Dual Closed-cell Stents
- The Clinical Presentation and Treatment of Distal Posterior Inferior Cerebellar artery Aneurysms: Report on 2 cases
