Pudendal nerve entrapment syndrome caused by ganglion cysts along the pudendal nerve
- Affiliations
-
- 1Department of Rehabilitation Medicine, Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea
- 2Department of Physical Medicine and Rehabilitation, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea
- KMID: 2515189
- DOI: http://doi.org/10.12701/yujm.2020.00437
Abstract
- Pudendal nerve entrapment (PNE) syndrome refers to the condition in which the pudendal nerve is entrapped or compressed. Reported cases of PNE associated with ganglion cysts are rare. Deep gluteal syndrome (DGS) is defined as compression of the sciatic or pudendal nerve due to a non-discogenic pelvic lesion. We report a case of PNE caused by compression from ganglion cysts and treated with steroid injection; we discuss this case in the context of DGS. A 77-year-old woman presented with a 3-month history of tingling and burning sensations in the left buttock and perineal area. Ultrasonography showed ganglion cystic lesions at the subgluteal space. Magnetic resonance imaging revealed cystic lesions along the pudendal nerve from below the piriformis to the Alcock’s canal and a full-thickness tear of the proximal hamstring tendon. Aspiration of the cysts did not yield any material. We then injected steroid into the cysts, which resolved her symptoms. Steroid injection into a ganglion cyst should be considered as a treatment option for PNE caused by ganglion cysts.
Figure
-
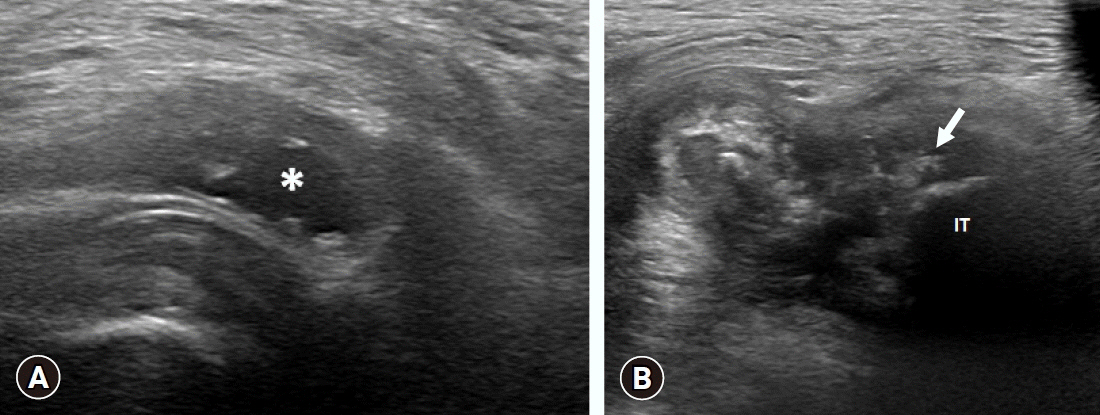
Fig. 1. Ultrasonographic findings. (A) A 2.6x1.2 cm-sized ganglion cystic lesion (asterisk) at the subgluteal space. (B) Full-thickness tear (arrow) of the proximal hamstring tendon at the ischial tuberosity (IT).
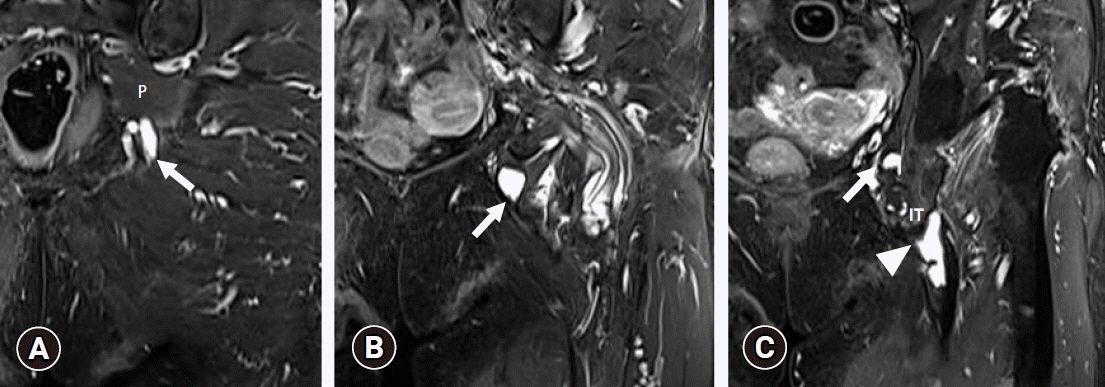
Fig. 2. Coronal fat-suppressed T2-weighted images of ganglion cyst courses along the pudendal nerve. (A) A 2.0x0.8 cm-sized ganglion cyst (arrow) below piriformis (P). (B) A 1.8x1.4 cm-sized ganglion cyst (arrow) at the entrance of the Alcock’s canal. (C) A 1.0x0.75 cm-sized ganglion cyst (arrow) within the Alcock’s canal and full-thickness tear (arrowhead) of the proximal hamstring tendon at the ischial tuberosity (IT).
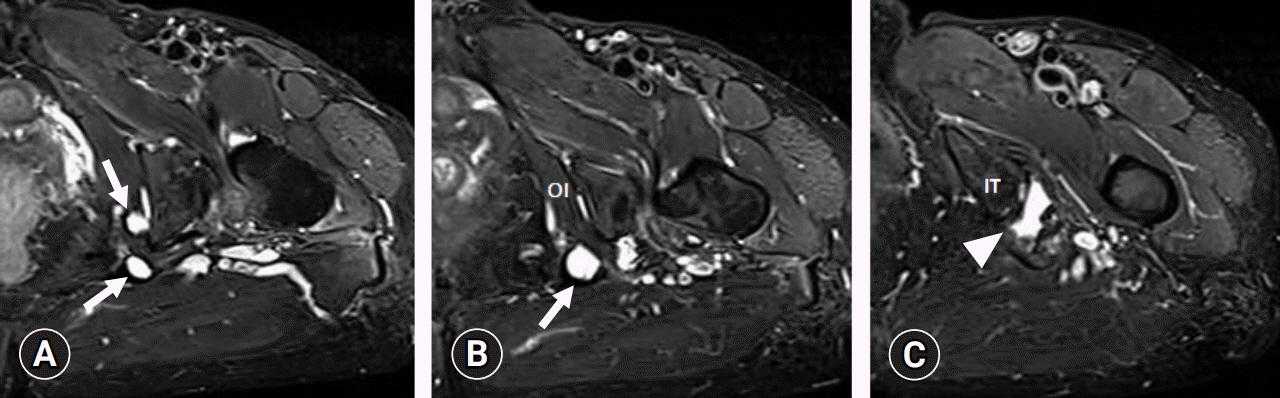
Fig. 3. Axial fat-suppressed T2-weighted images of ganglion cyst courses along the pudendal nerve. (A) A 1.0x0.8 cm-sized and 1.2x1.3 cm-sized ganglion cysts (arrows) around the Alcock’s canal. (B) A 1.3x1.5 cm-sized ganglion cyst (arrow) medial to the obturator internus (OI) muscle. (C) A full-thickness tear (arrowhead) of the proximal hamstring tendon at the ischial tuberosity (IT).
Reference
-
References
1. Ploteau S, Cardaillac C, Reina MA, Perrouin-Verbe E, Riant T, Labat JJ. Pudendal neuralgia due to pudendal nerve entrapment: warning signs observed in two cases and review of the literature. Pain Physician. 2016; 19:E449–54.2. Lee JW, Lee SM, Lee DG. pudendal nerve entrapment syndrome due to a ganglion cyst: a case report. Ann Rehabil Med. 2016; 40:741–4.
Article3. Alevizon SJ, Finan MA. Sacrospinous colpopexy: management of postoperative pudendal nerve entrapment. Obstet Gynecol. 1996; 88(4 Pt 2):713–5.
Article4. Pailhe R, Chiron P, Reina N, Cavaignac E, Lafontan V, Laffosse JM. Pudendal nerve neuralgia after hip arthroscopy: retrospective study and literature review. Orthop Traumatol Surg Res. 2013; 99:785–90.
Article5. Leibovitch I, Mor Y. The vicious cycling: bicycling related urogenital disorders. Eur Urol. 2005; 47:277–87.
Article6. Park JW, Lee YK, Lee YJ, Shin S, Kang Y, Koo KH. Deep gluteal syndrome as a cause of posterior hip pain and sciatica-like pain. Bone Joint J. 2020. 102-B:556–67.
Article7. Kaur J, Singh P. Pudendal nerve entrapment syndrome [Internet]. Treasure Island (FL): StatPearls Publishing;2020. [cited 2020 Jun 2]. https://www.ncbi.nlm.nih.gov/books/NBK544272/.8. Spinosa JP, de Bisschop E, Laurencon J, Kuhn G, Dubuisson JB, Riederer BM. Sacral staged reflexes to localize the pudendal compression: an anatomical validation of the concept. Rev Med Suisse. 2006; 2:2416–8. 2420–1.9. Itza Santos F, Salinas J, Zarza D, Gomez Sancha F, Allona Almagro A. Update in pudendal nerve entrapment syndrome: an approach anatomic-surgical, diagnostic and therapeutic. Actas Urol Esp. 2010; 34:500–9.10. Labat JJ, Riant T, Robert R, Amarenco G, Lefaucheur JP, Rigaud J. Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria). Neurourol Urodyn. 2008; 27:306–10.
Article11. Montoya TI, Calver L, Carrick KS, Prats J, Corton MM. Anatomic relationships of the pudendal nerve branches. Am J Obstet Gynecol. 2011; 205:504.
Article12. Gude W, Morelli V. Ganglion cysts of the wrist: pathophysiology, clinical picture, and management. Curr Rev Musculoskelet Med. 2008; 1:205–11.
Article13. Derbyshire RC. Observations on the treatment of ganglia with a report on hydrocortisone. Am J Surg. 1966; 112:635–6.
Article14. Devor M, Govrin-Lippmann R, Raber P. Corticosteroids suppress ectopic neural discharge originating in experimental neuromas. Pain. 1985; 22:127–37.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pudendal Nerve Entrapment Syndrome due to a Ganglion Cyst: A Case Report
- Intrapelvic Nerve Entrapment Syndrome Caused by a Variation of the Intrapelvic Piriformis Muscle and Abnormal Varicose Vessels: A Case Report
- Suprascapular nerve entrapment syndrome by a ganglion, treated with nonoperative method: a case report
- Ultrasound-guided pudendal nerve pulsed radiofrequency in patients with refractory pudendal neuralgia: Three cases report
- Entrapment Neuropathy of the Suprascapular Nerve by a Gangilion - A Case Report -
