Surgical Treatment of Comminuted Olecranon Fracture Using Locking Compression Plate Fixation
- Affiliations
-
- 1Department of Orthopaedic Surgery, Gyeongsang National University Hospital, Jinju, Korea
- 2Department of Orthopaedic Surgery, Gyeongsang National University Changwon Hospital, Changwon, Korea
- 3Department of Orthopaedic Surgery, Gyeongsang National University School of Medicine, Jinju, Korea
- 4Institute of Health Science, Gyeongsang National University, Jinju, Korea
- KMID: 2513202
- DOI: http://doi.org/10.12790/ahm.20.0078
Abstract
- Purpose
Several types of surgical methods from tension band wiring to plate fixation are used in olecranon fractures. In comminuted olecranon fractures, plate fixation is recommended as it is difficult to obtain stable fixation of the bone fragments and joint congruency. The authors performed operations using compression locking plate for olecranon fractures corresponding to Mayo classification IIB and IIIB, and report the radiologic and functional results.
Methods
Twenty-one patients who underwent plate fixation surgery for comminuted olecranon fractures at our hospital from September 2011 to April 2019 were enrolled in this study. Patients were retrospectively analyzed for at least 1 year. The classification of olecranon fracture was performed using the Mayo classification. For the analysis of the postoperative results, radiological union time, postoperative range of motion, complications, and functional results based on Mayo elbow performance score (MEPS) were evaluated.
Results
The union was achieved in all cases and three posttraumatic arthritis were observed at the final follow-up. The average range of motion was 134.3° in flexion, –9.8° in extension. The mean MEPS was 93.1. There was no statistically significant difference in MEPS between the group that used technique of interfragmentary fixation and the group that did not (p=0.534).
Conclusion
Surgical treatment using a locking compression plate fixation in comminuted olecranon fracture resulted in excellent functional results. Restoration of articular surface using Kirschner wire or interfragmentary screw between small bone fragments is considered a useful method for obtaining good functional results.
Figure
-
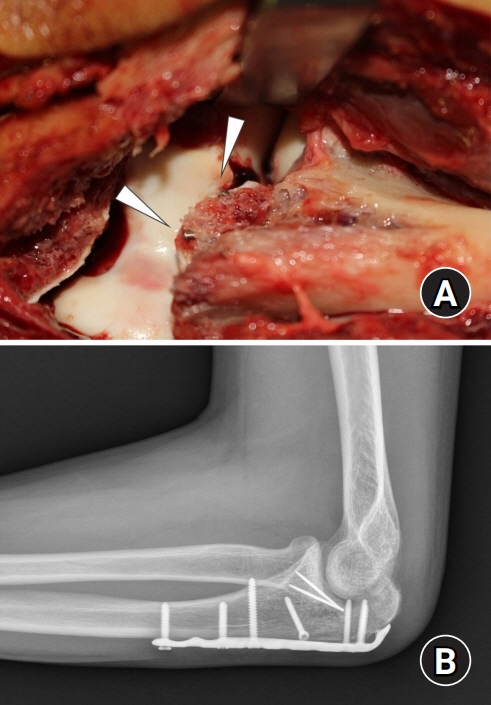
Fig. 1. Intraoperative photo shows Kirschner wire tips (arrowheads) for interfragmentary fixation of articular fragments (A). Lateral radiographs present a satisfactory reduction of articular surface with interfragmentary fixation (B).
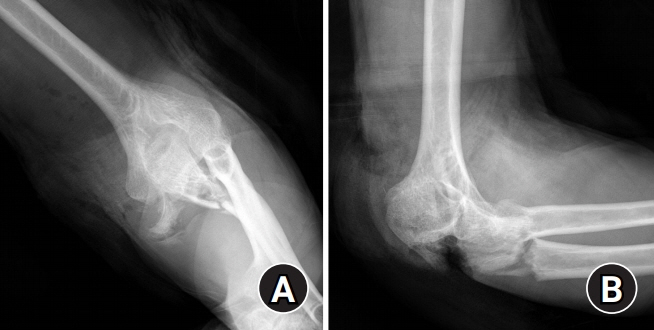
Fig. 2. Radiographs of the severe comminuted fracture of left olecranon due to industrial injury in a 60 year-old man (case 11). (A) Anteroposterior view. (B) Lateral view.
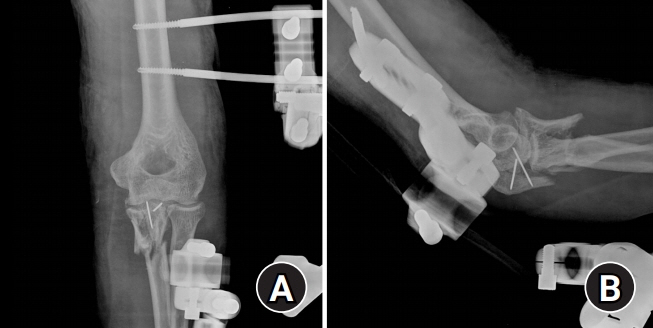
Fig. 3. Radiographs after emergency surgery with external fixation and temporary fixation of articular fragments. (A) Anteroposterior view. (B) Lateral view.

Fig. 4. Radiographs after conversion open reduction and internal fixation with plate, interfragmentary screw fixation and cerclage wiring. Radiographs (A, anteroposterior view; B, lateral view) show satisfactory reduction of articular congruency.
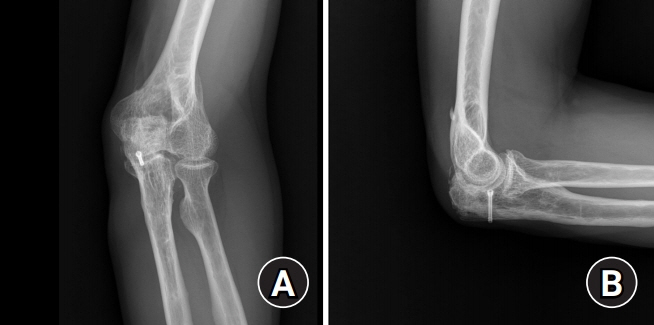
Fig. 5. At 18 months after conversion open reduction and internal fixation, radiographs (A, anteroposterior view; B, lateral view) show the remnant headless compression screw for articular fragment fixation and minimal posttraumatic arthritis of ulnohumeral joint.

Fig. 6. At 18 months after surgery, clinical pictures present no significant limitation of elbow motion of patient. (A) Flexion of elbow, (B) extension of elbow, and (C) 15° of flexion contracture of the injured elbow.
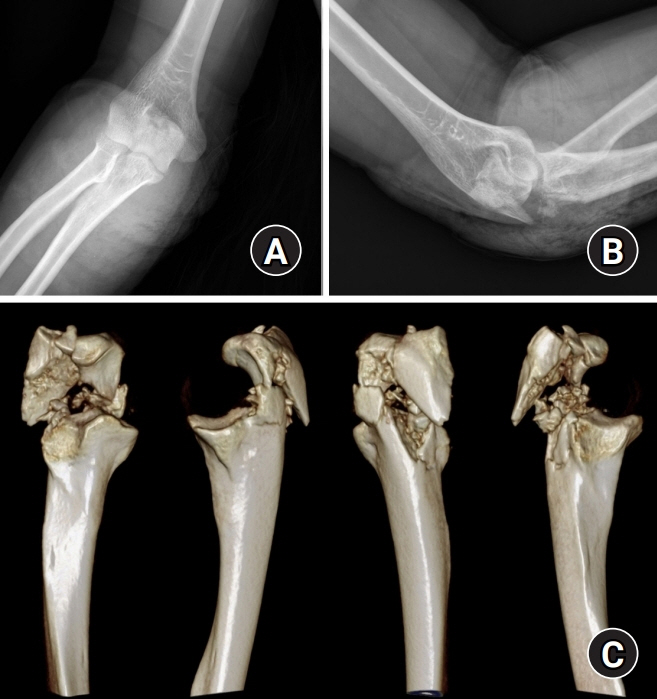
Fig. 7. Radiographs (A, anteroposterior view; B, lateral view) show a comminuted fracture of the right elbow in a 19-year-old male patient (case 20). (C) Three-dimensional computed tomography images present severe comminution of olecranon fracture including articular surface.
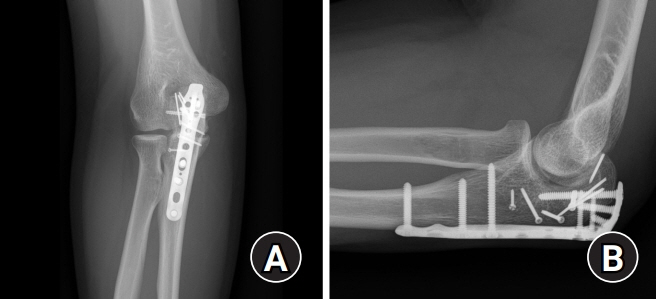
Fig. 8. At 1 year after surgery, radiographs (A, anteroposterior view; B, lateral view) show the satisfactory reduction of ulnohumeral joint using the plate and screws with intrefragmentary fixation.
Reference
-
1. Veillette CJ, Steinmann SP. Olecranon fractures. Orthop Clin North Am. 2008; 39:229–36.
Article2. Hong IT, Jung K, Kim YS, Han SH. The result of locking compression plate olecranon plate fixation for unstable comminuted olecranon fracture. Arch Hand Micro. 2019; 24:133–41.
Article3. Fan GF, Wu CC, Shin CH. Olecranon fractures treated with tension band wiring techniques: comparisons among three different configurations. Changgeng Yi Xue Za Zhi. 1993; 16:231–8.4. Hume MC, Wiss DA. Olecranon fractures: a clinical and radiographic comparison of tension band wiring and plate fixation. Clin Orthop Relat Res. 1992; (285):229–35.5. Chalidis BE, Sachinis NC, Samoladas EP, Dimitriou CG, Pournaras JD. Is tension band wiring technique the “gold standard” for the treatment of olecranon fractures?: a long term functional outcome study. J Orthop Surg Res. 2008; 3:9.
Article6. Murphy DF, Greene WB, Dameron TB Jr. Displaced olecranon fractures in adults: clinical evaluation. Clin Orthop Relat Res. 1987; (224):215–23.
Article7. Powell AJ, Farhan-Alanie OM, Bryceland JK, Nunn T. The treatment of olecranon fractures in adults. Musculoskelet Surg. 2017; 101:1–9.
Article8. Ali M, Hatzantonis C, Aspros D, Joshi N, Clark DI, Tambe A. Management of type IIB and IIIB olecranon fractures: case series. Int J Surg Case Rep. 2017; 41:296–300.
Article9. Shin HD, Yang JH, Kim PS. Internal fixation using double plates for comminuted olecranon fractures in adults. J Korean Fract Soc. 2009; 22:166–71.
Article10. Wilson J, Bajwa A, Kamath V, Rangan A. Biomechanical comparison of interfragmentary compression in transverse fractures of the olecranon. J Bone Joint Surg Br. 2011; 93:245–50.
Article11. De Giacomo AF, Tornetta P 3rd, Sinicrope BJ, et al. Outcomes after plating of olecranon fractures: a multicenter evaluation. Injury. 2016; 47:1466–71.
Article12. Mellema JJ, Lindenhovius AL, Jupiter JB. The posttraumatic stiff elbow: an update. Curr Rev Musculoskelet Med. 2016; 9:190–8.
Article13. Inui A, Kuroda T, Kurosawa T, et al. Case series of comminuted olecranon fracture treated by plate fixation; do we have to remove the plate? Kobe J Med Sci. 2018; 64:E115–8.14. Bailey CS, MacDermid J, Patterson SD, King GJ. Outcome of plate fixation of olecranon fractures. J Orthop Trauma. 2001; 15:542–8.
Article15. Macko D, Szabo RM. Complications of tension-band wiring of olecranon fractures. J Bone Joint Surg Am. 1985; 67:1396–401.
Article16. Tejwani NC, Garnham IR, Wolinsky PR, Kummer FJ, Koval KJ. Posterior olecranon plating: biomechanical and clinical evaluation of a new operative technique. Bull Hosp Jt Dis. 2002-2003; 61:27–31.17. Hong CC, Nashi N, Hey HW, Chee YH, Murphy D. Clinically relevant heterotopic ossification after elbow fracture surgery: a risk factors study. Orthop Traumatol Surg Res. 2015; 101:209–13.
Article18. Mielants H, Vanhove E, de Neels J, Veys E. Clinical survey of and pathogenic approach to para-articular ossifications in long-term coma. Acta Orthop Scand. 1975; 46:190–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Result of Locking Compression Plate Olecranon Plate Fixation for Unstable Comminuted Olecranon Fracture
- Treatment of Femur Supracondylar Fracture with Locking Compression Plate
- Medial Plating of Distal Femoral Fracture with Locking Compression Plate-Proximal Lateral Tibia: Cases' Report
- Functional Results of Olecranon Fracture-Dislocation According to the Methods of Internal Fixation
- Failure of Distal Locking Screws in an Intraarticular Distal Radius Fracture Treated with Volar Locking Plate Fixation
