J Korean Med Sci.
2021 Feb;36(6):e34. 10.3346/jkms.2021.36.e34.
Validation of Olfactory Questionnaire in Koreans: an Alternative for Conventional Psychophysical Olfactory Tests
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- 2Department of Biomedical Engineering, Seoul National University College of Medicine, Seoul, Korea
- KMID: 2512629
- DOI: http://doi.org/10.3346/jkms.2021.36.e34
Abstract
- Background
The patients with coronavirus disease 2019 (COVID-19), a worldwide pandemic infection, frequently complain of olfactory disorders. However, psychophysical olfactory tests performed by an examiner are very difficult in these highly infectious patients. This study aimed to develop and validate a questionnaire for olfactory function that can be readily used to evaluate olfactory loss.
Methods
Fourteen smell-related questions were created based on smells familiar to Koreans. Among them, questions with a κ value of 0.6 or higher were finally selected through a test-retest reliability analysis. The correlations between the scores of the olfactory questionnaire and those of olfactory function tests (Butanol Threshold Test [BTT] and Cross Cultural Smell Identification Test [CCSIT]) were analyzed. To evaluate the predictive ability of the questionnaire and elicit cutoff values, receiver operating characteristic (ROC) curves were generated.
Results
Out of the 14 questions in the questionnaire, 11 (κ > 0.6) were selected for the olfactory questionnaire. We analyzed 2,273 subjects, and there was a significant correlation between the total score of the olfactory questionnaire and the BTT (r = 0.643, P < 0.001) or CCSIT (r = 0.615, P < 0.001) scores. ROC curves for the olfactory questionnaire, BTT, and CCSIT all demonstrated high predictive power to discriminate anosmia and severe hyposmia from normosmia. Regarding mild to moderate hyposmia, however, ROC curve for the olfactory questionnaire alone showed high predictive power of discrimination from normosmia. Based on the results of ROC curves among the subclasses, we suggest the classification of the total score of the questionnaire as 0–4, 5–17, 18–27, 28–41, and 42–44, for anosmia, severe hyposmia, moderate hyposmia, mild hyposmia, and normosmia, respectively.
Conclusion
The total scores of the questionnaires correlated with the BTT and CCSIT scores. The symptom questionnaire for olfactory dysfunction may be useful as an alternative tool for olfactory function testing, when unavailable.
Figure
-
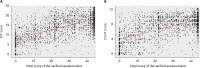
Fig. 1 Correlation between total score of the verified questionnaire and (A) the BTT score and (B) CCSIT score.BTT = Butanol Threshold Test, CCSIT = Cross Cultural Smell Identification Test.

Fig. 2 ROC curves for the total score of the olfactory questionnaire, BTT and CCSIT scores to predict the four levels of olfactory dysfunction from normosmia: (A) anosmia, (B) severe hyposmia, (C) moderate hyposmia, and (D) mild hyposmia. The self-rating scale for olfactory dysfunction is used as a reference. The predictive ability is calculated based on the AUC.ROC = receiver operating characteristic, BTT = Butanol Threshold Test, CCSIT = Cross Cultural Smell Identification Test, AUC = area under the curve.
Reference
-
1. Hong SM, Park IH, Kim KM, Shin JM, Lee HM. Relationship between the Korean version of the Sniffin' Stick Test and the T&T olfactometer in the Korean population. Clin Exp Otorhinolaryngol. 2011; 4(4):184–187. PMID: 22232713.2. Kim JM, Jeong MS, Shin DH, Seol JH, Hong SC, Cho JH, et al. Olfactory identification test using familiar distracters for Koreans. Clin Exp Otorhinolaryngol. 2014; 7(1):19–23. PMID: 24587876.
Article3. Park CW, Do NY, Rha KS, Chung SM, Kwon YJ. Korean Academy of Medical Sciences. Development of guideline for rating the physical impairment of otolaryngologic field. J Korean Med Sci. 2009; 24(Suppl 2):S258–S266. PMID: 19503682.
Article4. Doty RL, Shaman P, Kimmelman CP, Dann MS. University of Pennsylvania Smell Identification Test: a rapid quantitative olfactory function test for the clinic. Laryngoscope. 1984; 94(2 Pt 1):176–178. PMID: 6694486.
Article5. Hummel T, Sekinger B, Wolf SR, Pauli E, Kobal G. ‘Sniffin' sticks’: olfactory performance assessed by the combined testing of odor identification, odor discrimination and olfactory threshold. Chem Senses. 1997; 22(1):39–52. PMID: 9056084.6. Takagi SF. A standardized olfactometer in Japan. A review over ten years. Ann N Y Acad Sci. 1987; 510(1):113–118. PMID: 3481235.7. Cain WS, Gent J, Catalanotto FA, Goodspeed RB. Clinical evaluation of olfaction. Am J Otolaryngol. 1983; 4(4):252–256. PMID: 6625103.
Article8. Doty RL, Marcus A, Lee WW. Development of the 12‐item cross‐cultural smell identification test (CC‐SIT). Laryngoscope. 1996; 106(3 Pt 1):353–356. PMID: 8614203.9. Lechien JR, Chiesa-Estomba CM, De Siati DR, Horoi M, Le Bon SD, Rodriguez A, et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Eur Arch Otorhinolaryngol. 2020; 277(8):2251–2261. PMID: 32253535.
Article10. Eliezer M, Hautefort C, Hamel AL, Verillaud B, Herman P, Houdart E, et al. Sudden and complete olfactory loss function as a possible symptom of covid-19. JAMA Otolaryngol Head Neck Surg. 2020; 146(7):674–675. PMID: 32267483.11. Gane SB, Kelly C, Hopkins C. Isolated sudden onset anosmia in COVID-19 infection. A novel syndrome? Rhinology. 2020; 58(3):299–301. PMID: 32240279.
Article12. Hopkins C, Surda P, Kumar N. Presentation of new onset anosmia during the COVID-19 pandemic. Rhinology. 2020; 58(3):295–298. PMID: 32277751.
Article13. Lee Y, Min P, Lee S, Kim SW. Prevalence and duration of acute loss of smell or taste in COVID-19 patients. J Korean Med Sci. 2020; 35(18):e174. PMID: 32383370.
Article14. Takebayashi H, Tsuzuki K, Oka H, Fukazawa K, Daimon T, Sakagami M. Clinical availability of a self-administered odor questionnaire for patients with olfactory disorders. Auris Nasus Larynx. 2011; 38(1):65–72. PMID: 20594785.
Article15. Frasnelli J, Hummel T. Olfactory dysfunction and daily life. Eur Arch Otorhinolaryngol. 2005; 262(3):231–235. PMID: 15133691.
Article16. Nordin S, Brämerson A, Murphy C, Bende M. A Scandinavian adaptation of the Multi-Clinic Smell and Taste Questionnaire: evaluation of questions about olfaction. Acta Otolaryngol. 2003; 123(4):536–542. PMID: 12809108.
Article17. Langstaff L, Pradhan N, Clark A, Boak D, Salam M, Hummel T, et al. Validation of the olfactory disorders questionnaire for English-speaking patients with olfactory disorders. Clin Otolaryngol. 2019; 44(5):715–728. PMID: 31038840.
Article18. Zou L, Linden L, Cuevas M, Metasch ML, Welge‐Lüssen A, Hähner A, et al. Self‐reported mini olfactory questionnaire (Self‐MOQ): a simple and useful measurement for the screening of olfactory dysfunction. Laryngoscope. 2019.
Article19. Seok J, Shim YJ, Rhee CS, Kim JW. Correlation between olfactory severity ratings based on olfactory function test scores and self-reported severity rating of olfactory loss. Acta Otolaryngol. 2017; 137(7):750–754. PMID: 28112015.
Article20. Bujang MA, Baharum N. Guidelines of the minimum sample size requirements for Kappa agreement test. Epidemiol Biostat Public Health. 2017; 14(2):e12267.21. Cohen J. A coefficient of agreement for nominal scales. Educ Psychol Meas. 1960; 20(1):37–46.
Article22. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977; 33(1):159–174. PMID: 843571.
Article23. Flack VF, Afifi A, Lachenbruch P, Schouten H. Sample size determinations for the two rater kappa statistic. Psychometrika. 1988; 53(3):321–325.
Article24. Meng XL, Rosenthal R, Rubin DB. Comparing correlated correlation coefficients. Psychol Bull. 1992; 111(1):172–175.
Article25. Moein ST, Hashemian SM, Mansourafshar B, Khorram-Tousi A, Tabarsi P, Doty RL. Smell dysfunction: a biomarker for COVID-19. Int Forum Allergy Rhinol. 2020; 10(8):944–950. PMID: 32301284.
Article26. Choi HG, Lee HJ, Shin HW, Lee JM, Lee CH, Mo JH, et al. Correlation between olfactory threshold test, olfactory identification test and subjective symptoms. Korean J Otorhinolaryngol-Head Neck Surg. 2008; 51(11):1015–1019.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Olfactory Threshold Tests:CCCRC Test versus Step Method
- The Current Status of Evaluation Technologies for the Function of Human Olfaction
- Clinical Feasibility of Scent Survey for Screening Test for Olfactory Function
- Clinical Diagnosis and Treatment of Olfactory Dysfunction
- Selection of Olfactory Identification Items for Koreans
