Diabetic Muscle Infarction in a Young Patient with Prader-Willi Syndrome and Type 2 Diabetes Mellitus
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- 2Division of Endocinology, Depatment of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- 3Division of Rheumatology, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- KMID: 2511892
- DOI: http://doi.org/10.4093/jkd.2020.21.4.227
Abstract
- Diabetic muscle infarction (DMI), also known as diabetic myonecrosis, is a rare complication of diabetes mellitus (DM); hence, it is often underdiagnosed. Thus, timely diagnosis and treatment are essential for a better prognosis. We describe a 24-year-old woman with Prader-Willi syndrome and an 8-year history of uncontrolled type 2 DM, who presented with a sudden onset of fever and subacute painful swelling of her left thigh. She was finally diagnosed with DMI based on magnetic resonance imaging and muscle biopsy after excluding other infectious and inflammatory diseases of proximal muscles. The patient was treated with bed rest, strict glycemic control, and analgesics, and her symptoms gradually resolved. DMI should be considered in the differential diagnosis of patients with poorly controlled DM, who present with subacute pain and swelling of lower extremity muscles, without a history of trauma.
Figure
-
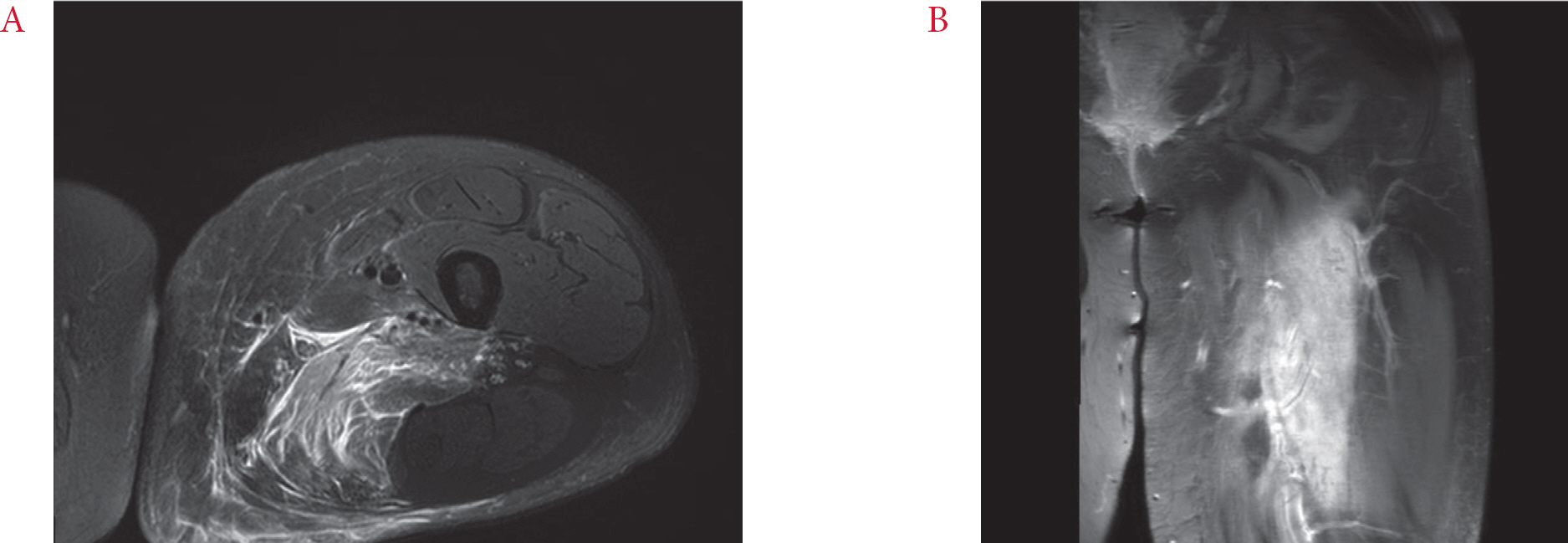
Fig. 1. Magnetic resonance imaging of left thigh. (A) Axial T2-weighted image with fat suppression, demonstrating enlargement and diffusely increased signal intensity of the adductor magnus muscle and irregular hypointense area at the center. (B) Coronal T1-weighted, fat-suppressed image with gadolinium enhancement.

Fig. 2. Diabetic muscle infarction involving the left thigh showing its enlargement compared with the right thigh.

Fig. 3. (A∼C) Biopsy of the left thigh skeletal muscle showing multifocal necrosis of muscle fibers and dens interstitial infiltration of neutrophils and lymphocytes, and panniculitis. H&E stain, ×100; ×200; ×200, respectively. (D∼F) Gram stain, Wright-Giemsa stain, and Periodic acid Schiff stain for detecting bacteria and fungus were negative. ×200.
Reference
-
1. Angervall L., Stener B. Tumoriform focal muscular degeneration in two diabetic patients. Diabetologia. 1965. 1:39–42.
Article2. Horton WB., Taylor JS., Ragland TJ., Subauste AR. Diabetic muscle infarction: a systematic review. BMJ Open Diabetes Res Care. 2015. 3:e000082.
Article3. Lentine KL., Guest SS. Diabetic muscle infarction in end-stage renal disease. Nephrol Dial Transplant. 2004. 19:664–9.
Article4. Chawla A., Dubey N., Chew KM., Singh D., Gaikwad V., Peh WC. Magnetic resonance imaging of painful swollen legs in the emergency department: a pictorial essay. Emerg Radiol. 2017. 24:577–84.
Article5. Jelinek JS., Murphey MD., Aboulafia AJ., Dussault RG., Kaplan PA., Snearly WN. Muscle infarction in patients with diabetes mellitus: MR imaging findings. Radiology. 1999. 211:241–7.
Article6. Kattapuram TM., Suri R., Rosol MS., Rosenberg AE., Kattapuram SV. Idiopathic and diabetic skeletal muscle necrosis: evaluation by magnetic resonance imaging. Skeletal Radiol. 2005. 34:203–9.
Article7. Chaussé G., Abikhzer G. The role of FDG PET in diabetic myonecrosis: a rare and underrecognized complication of diabetes. Clin Nucl Med. 2018. 43:112–3.8. Chester CS., Banker BQ. Focal infarction of muscle in diabetics. Diabetes Care. 1986. 9:623–30.
Article9. Silberstein L., Britton KE., Marsh FP., Raftery MJ., D’Cruz D. An unexpected cause of muscle pain in diabetes. Ann Rheum Dis. 2001. 60:310–2.
Article10. Umpierrez GE., Stiles RG., Kleinbart J., Krendel DA., Watts NB. Diabetic muscle infarction. Am J Med. 1996. 101:245–50.
Article11. Bjornskov EK., Carry MR., Katz FH., Lefkowitz J., Ringel SP. Diabetic muscle infarction: a new perspective on pathogenesis and management. Neuromuscul Disord. 1995. 5:39–45.
Article12. Yong TY., Khow KSF. Diabetic muscle infarction in end-stage renal disease: a scoping review on epidemiology, diagnosis and treatment. World J Nephrol. 2018. 7:58–64.
Article13. Yoon YS., Choi JL., Yu KP., Kwak SH., Kim JY. Diabetic muscle infarction in a chronic stroke patient: a case report. J Korean Acad Rehabil Med. 2010. 34:771–6.14. Yu HM., Jin HY., Park TS. Case of recurrent diabetic muscle infarction related to strict blood glucose control. Korean J Med. 2013. 84:737–41.
Article15. Lee HJ., Kim HJ., Hwang SY., Kim MK., Kwon HS., Baek KH, et al. A case of bilateral diffuse diabetic muscle infarction of the thighs in a patient with good glucose control. J Korean Diabetes. 2016. 17:67–72.
Article16. Tsuchiya T., Oto Y., Ayabe T., Obata K., Murakami N., Nagai T. Characterization of diabetes mellitus in Japanese Prader-Willi syndrome. Clin Pediatr Endocrinol. 2011. 20:33–8.
Article17. Bassali R., Hoffman WH., Chen H., Tuck-Muller CM. Hyperlipidemia, insulin-dependent diabetes mellitus, and rapidly progressive diabetic retinopathy and nephropathy in Prader-Willi syndrome with del(15)(q11.2q13). Am J Med Genet. 1997. 71:267–70.
Article18. Passone CBG., Pasqualucci PL., Franco RR., Ito SS., Mattar LBF., Koiffmann CP, et al. Prader-Willi syndrome: what is the general pediatrician supposed to do? – a review. Rev Paul Pediatr. 2018. 36:345–52.
