Clin Endosc.
2020 Nov;53(6):698-704. 10.5946/ce.2019.203.
Quality Indicators for the Detection of Helicobacter pylori-Negative Early Gastric Cancer: A Retrospective Observational Study
- Affiliations
-
- 1Koganei Tsurukame Clinic, Endoscopy Center, Tokyo, Japan
- 2Shinjuku Tsurukame Clinic, Digestive Disease Center, Tokyo, Japan
- 3Mirraza Shinjuku Tsurukame Clinic, Tokyo, Japan
- KMID: 2511229
- DOI: http://doi.org/10.5946/ce.2019.203
Abstract
- Background/Aims
While Helicobacter pylori (HP)-negative gastric cancer is frequently reported, little is known about the predictors for detecting HP-negative early gastric cancer (EGC). We aimed to evaluate the predictors for the detection of HP-negative EGC.
Methods
We retrospectively reviewed 13,477 consecutive asymptomatic cases where upper endoscopy was performed by nine physicians from April 2017 to March 2019 and analyzed the detection rate of high-risk lesions (HRLs), including EGC, tubular adenoma, and lymphoma, according to the status of HP infection. The observation time was corrected for multiple regression analyses.
Results
For all physicians, the average observation time for screening HP-eradicated and -naïve patients was shorter than that for screening HP-positive patients (p<0.05). Multiple regression analyses revealed that the observation time in the three groups was an independent predictor for detecting HRLs in HP-eradicated patients (p=0.03106, 0.01263, and 0.02485, respectively), while experience of endoscopy was an independent predictor for detecting HRLs in HP-naïve patients (p=0.02638).
Conclusions
While observation time during screening endoscopy was a quality indicator for detecting HRLs in HP-eradicated patients, experience of endoscopy was a quality indicator for detecting HRLs in HP-naïve patients.
Figure
-
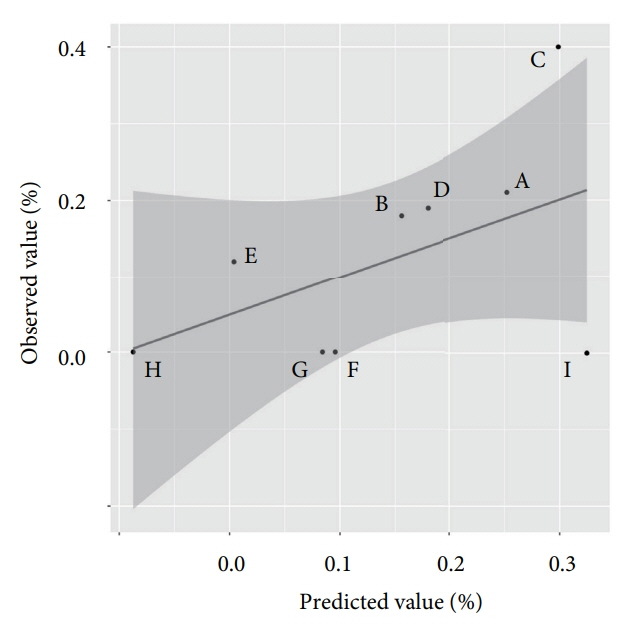
Fig. 1. Observed-predicted plot of the detection rate of Helicobacter pylori (HP)-naïve high-risk lesions (HRLs). On the basis of the equation calculated by multivariate analysis, a black line was drawn for the prediction of the physicians’ detection rate of HP-naïve HRLs. The grey area indicates the 95% confidence interval. Each dot plot indicates the actual physicians’ detection rate of HP-naïve HRLs.
Cited by 1 articles
-
Quality Indicator for Gastric Cancer Detection Based on
Helicobacter pylori Status
Jae Myung Park
Clin Endosc. 2020;53(6):629-630. doi: 10.5946/ce.2020.270.
Reference
-
1. Nomura A, Stemmermann GN, Chyou P-H, Kato I, Perez-Perez GI, Blaser MJ. Helicobacter pylori infection and gastric carcinoma among Japanese Americans in Hawaii. N Engl J Med. 1991; 325:1132–1136.2. Helicobacter and Cancer Collaborative Group. Gastric cancer and Helicobacter pylori: a combined analysis of 12 case control studies nested within prospective cohorts. Gut. 2001; 49:347–353.3. Moss SF. The clinical evidence linking Helicobacter pylori to gastric cancer. Cell Mol Gastroenterol Hepatol. 2017; 3:183–191.4. Uemura N, Okamoto S, Yamamoto S, et al. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med. 2001; 345:784–789.5. Wong BC, Lam SK, Wong WM, et al. Helicobacter pylori eradication to prevent gastric cancer in a high-risk region of China: a randomized controlled trial. JAMA. 2004; 291:187–194.6. Fuccio L, Zagari RM, Eusebi LH, et al. Meta-analysis: can Helicobacter pylori eradication treatment reduce the risk for gastric cancer? Ann Intern Med. 2009; 151:121–128.7. Yamamoto Y, Fujisaki J, Omae M, Hirasawa T, Igarashi M. Helicobacter pylori-negative gastric cancer: characteristics and endoscopic findings. Dig Endosc. 2015; 27:551–561.8. Kobayashi M, Sato Y, Terai S. Endoscopic surveillance of gastric cancers after Helicobacter pylori eradication. World J Gastroenterol. 2015; 21:10553–10562.9. Wang C, Yuan Y, Hunt RH. The association between Helicobacter pylori infection and early gastric cancer: a meta-analysis. Am J Gastroenterol. 2007; 102:1789–1798.10. Matsuo T, Ito M, Takata S, Tanaka S, Yoshihara M, Chayama K. Low prevalence of Helicobacter pylori-negative gastric cancer among Japanese. Helicobacter. 2011; 16:415–419.11. Ueyama H, Matsumoto K, Nagahara A, Hayashi T, Yao T, Watanabe S. Gastric adenocarcinoma of the fundic gland type (chief cell predominant type). Endoscopy. 2014; 46:153–157.
Article12. Ishibashi F, Fukushima K, Ito T, Kobayashi K, Tanaka R, Onizuka R. Influence of Helicobacter pylori infection on endoscopic findings of gastric adenocarcinoma of the fundic gland type. J Gastric Cancer. 2019; 19:225–233.13. Saka A, Yagi K, Nimura S. Endoscopic and histological features of gastric cancers after successful Helicobacter pylori eradication therapy. Gastric Cancer. 2016; 19:524–530.14. Hamashima C, Ogoshi K, Okamoto M, Shabana M, Kishimoto T, Fukao A. A community-based, case-control study evaluating mortality reduction from gastric cancer by endoscopic screening in Japan. PLoS One. 2013; 8:e79088.
Article15. Hamashima C, Ogoshi K, Narisawa R, et al. Impact of endoscopic screening on mortality reduction from gastric cancer. World J Gastroenterol. 2015; 21:2460–2466.
Article16. Hamashima C, Shabana M, Okada K, Okamoto M, Osaki Y. Mortality reduction from gastric cancer by endoscopic and radiographic screening. Cancer Sci. 2015; 106:1744–1749.
Article17. Teh JL, Tan JR, Lau LJ, et al. Longer examination time improves detection of gastric cancer during diagnostic upper gastrointestinal endoscopy. Clin Gastroenterol Hepatol. 2015; 13:480–487.e2.
Article18. Kawamura T, Wada H, Sakiyama N, et al. Examination time as a quality indicator of screening upper gastrointestinal endoscopy for asymptomatic examinees. Dig Endosc. 2017; 29:569–575.
Article19. Park JM, Huo SM, Lee HH, Lee BI, Song HJ, Choi MG. Longer observation time increases proportion of neoplasms detected by esophagogastroduodenoscopy. Gastroenterology. 2017; 153:460–469.e1.
Article20. Januszewicz W, Wieszczy P, Bialek A, et al. Endoscopist biopsy rate as a quality indicator for outpatient gastroscopy: a multicenter cohort study with validation. Gastrointest Endosc. 2019; 89:1141–1149.
Article21. Kimura K, Takemoto T. An endoscopic recognition of the atrophic border and its significance in chronic gastritis. Endoscopy. 1969; 1:87–97.
Article22. R Core Team. R: a language and environment for statistical computing. R foundation for statistical computing [Internet]. Vienna: The R Foundation;c2018. [cited 2019 Jan 12]. Available from: https://www.R-project.org/.23. Veitch AM, Uedo N, Yao K, East JE. Optimizing early upper gastrointestinal cancer detection at endoscopy. Nat Rev Gastroenterol Hepatol. 2015; 12:660–667.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Helicobacter pylori-negative Gastric Cancer
- Prevention of Gastric Cancer: Helicobacter pylori Treatment
- Current Evidence for a Paradigm Shift in Gastric Cancer Prevention From Endoscopic Screening to Helicobacter pylori Eradication in Korea
- Helicobacter pylori Eradication and Gastric Cancer Prevention
- Effectiveness of Helicobacter pylori Eradication before Endoscopic Resection
