Intraoperative monitoring of somatosensory and visual evoked potentials for detecting posterior cerebral artery infarction during anteromesial temporal resection
- Affiliations
-
- 1Wonkwang University School of Medicine, Iksan, Korea
- 2Department of Neurology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2511085
- DOI: http://doi.org/10.14253/acn.2020.22.2.104
Abstract
- We performed intraoperative neurophysiological monitoring (INM) during anteromesial temporal resection (AMTR) in a patient with lesional temporal lobe epilepsy. INM revealed a sudden decrease in N20 waves in somatosensory evoked potentials (SSEPs) and poor P100 waves in visual evoked potentials (VEPs). These changes developed after applying electrocoagulation in the right mesial temporal areas. Postoperative brain magnetic resonance imaging demonstrated right thalamic and medial occipital infarctions. SSEPs and VEPs monitoring can be useful for detecting posterior cerebral artery infarction in AMTR.
Keyword
Figure
-
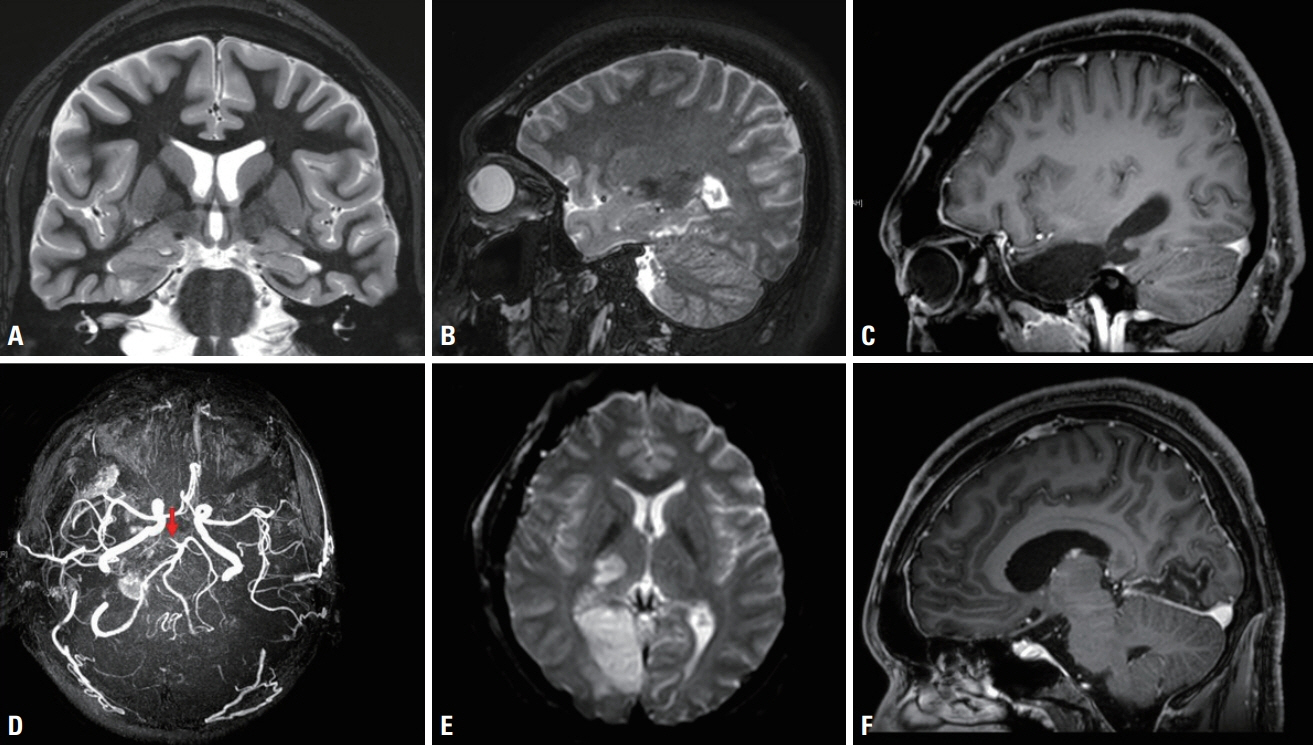
Fig. 1. Pre- and postoperative magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) findings. (A, B) Preoperative T2-weighted oblique coronal and sagittal MRI images show an enlarged right parahippocampal gyrus with cystic changes and a malformed cortex that extend up to the tail of the hippocampus. (C) Postoperative T1-weighted sagittal MRI image shows removal of the right anteromesial temporal regions including the tumor, amygdala, and hippocampus. (D) MRA image reveals occlusion of the P1 part of the right posterior cerebral artery (PCA, arrow). (E, F) Diffusion-weighted axial and T1-weighted sagittal MRI images demonstrate ischemic lesions in the lateral part of the right thalamus as well as the mesial part of the right occipital gyrus, indicating right PCA infarction.
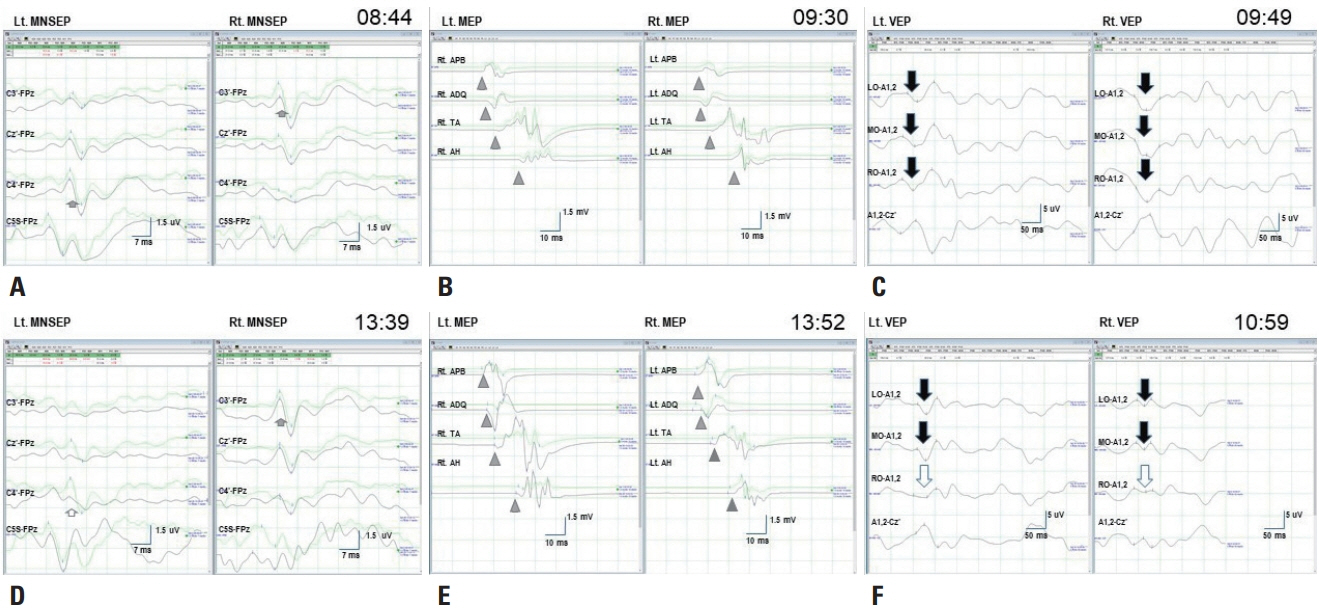
Fig. 2. Baseline and final data recordings. (A) Baseline median nerve somatosensory evoked potential (MNSEP) show a normal N20 waves (short arrows) for each stimulation. (B) Baseline transcranial electrical motor evoked potentials (MEPs) show polyphasic compound muscle action potentials (arrowheads) at the abductor pollicis brevis, abductor digiti quinti, tibialis anterior, and abductor hallucis for stimulation on each side. (C) Baseline visual evoked potentials (VEPs) show normal P100 waves (long arrows) in the left occipital (LO), middle occipital (MO), and right occipital (RO) channels for stimulation of each eye. (D) Final data for the left MNSEP reveal decreased N20 waves (hollow short arrow) in the C4’-FPz channel but no significant change in N20 waves (short arrow) in the C3’-FPz channel for the right MNSEP. (E) Final MEPs data show no significant changes (arrowheads) in any channels. (F) Final VEPs data reveal fair wave formation (hollow long arrow) for P100 waves in the RO-A1,2 channels but no significant changes in P100 waves (long arrows) in the LO or MO recordings for stimulation of either eye. Lt., left; Rt., right.
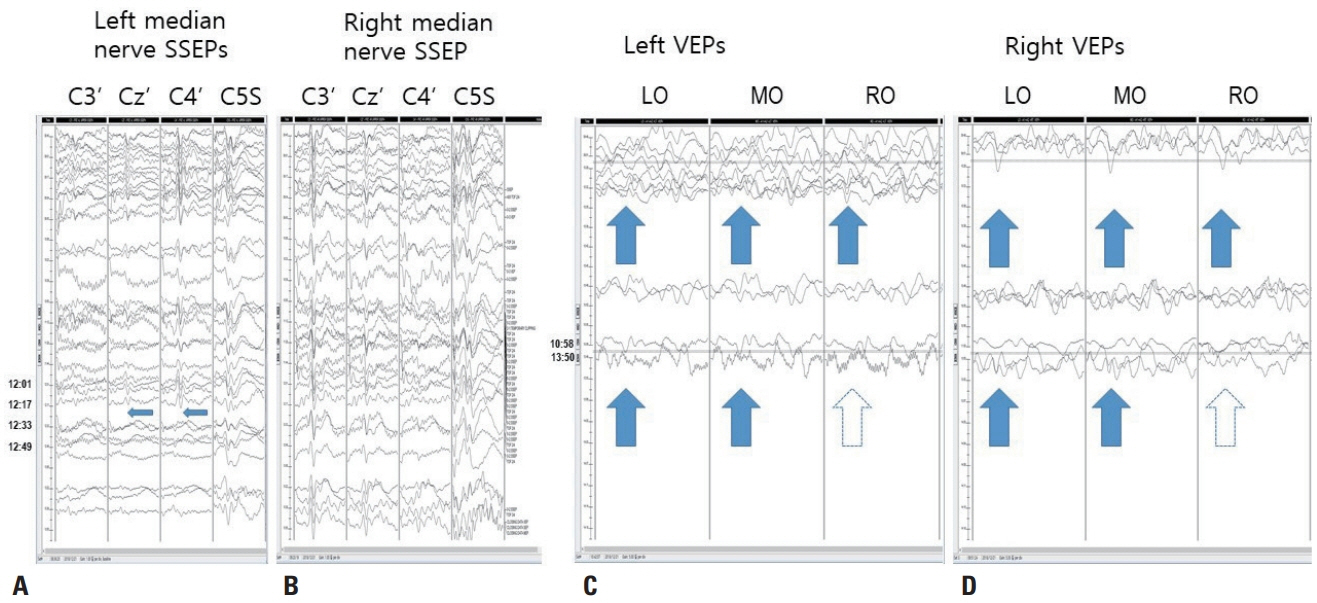
Fig. 3. Stacked results of somatosensory evoked potentials (SSEPs) and visual evoked potentials. (A) Left median nerve SSEPs. N20 waves at Cz’ and C4’ and the P14 wave at C5S are well formed in the baseline recordings (09:48, arrows), but the N20 waves abruptly disappear between 12:17 and 12:23 (narrow arrows), while the P14 wave continues, indicating central conduction defect above the spinal level. The vertical scale is 10 mV. (B) Right median nerve SSEPs. N20 waves at C3’ and C4’ and the P14 wave at C5S are well formed. The vertical scale is 10 mV. (C, D) Left and right visual evoked potentials (VEPs). The P100 waves at left occipital (LO), middle occipital (MO), and right occipital (RO) are fairly well formed from the beginning. From 13:50, the P100 wave at LO and MO are still seen (arrows), but that at RO is poorly formed (hollow arrows). The vertical scale is 5 mV.
Reference
-
1. Kim SM, Kim SH, Seo DW, Lee KW. Intraoperative neurophysiologic monitoring: basic principles and recent update. J Korean Med Sci. 2013; 28:1261–1269.
Article2. Koo DL, Lee WG, Hong SC, Seo DW. Clinical usefulness of intraoperative motor-evoked potential monitoring during temporal lobe epilepsy surgery. J Clin Neurol. 2019; 15:285–291.
Article3. Tebo CC, Evins AI, Christos PJ, Kwon J, Schwartz TH. Evolution of cranial epilepsy surgery complication rates: a 32-year systematic review and meta-analysis. J Neurosurg. 2014; 120:1415–1427.
Article4. Gooneratne IK, Mannan S, de Tisi J, Gonzalez JC, McEvoy AW, Miserocchi A, et al. Somatic complications of epilepsy surgery over 25 years at a single center. Epilepsy Res. 2017; 132:70–77.
Article5. Meyer KL, Dempsey RJ, Roy MW, Donaldson DL. Somatosensory evoked potentials as a measure of experimental cerebral ischemia. J Neurosurg. 1985; 62:269–275.
Article6. Thirumala PD, Udesh R, Muralidharan A, Thiagarajan K, Crammond DJ, Chang YF, et al. Diagnostic value of somatosensory-evoked potential monitoring during cerebral aneurysm clipping: a systematic review. World Neurosurg. 2016; 89:672–680.
Article7. Goto T, Tanaka Y, Kodama K, Kusano Y, Sakai K, Hongo K. Loss of visual evoked potential following temporary occlusion of the superior hypophyseal artery during aneurysm clip placement surgery. Case report. J Neurosurg. 2007; 107:865–867.8. Kodama K, Goto T, Sato A, Sakai K, Tanaka Y, Hongo K. Standard and limitation of intraoperative monitoring of the visual evoked potential. Acta Neurochir (Wien). 2010; 152:643–648.
Article9. Dekeyzer S, De Kock I, Nikoubashman O, Vanden Bossche S, Van Eetvelde R, De Groote J, et al. “Unforgettable” - a pictorial essay on anatomy and pathology of the hippocampus. Insights Imaging. 2017; 8:199–212.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Early Detection of the Internal Capsule Infarction by Intraoperative Neuromonitoring in Mesial Temporal Epilepsy Surgery
- Intraoperative Neurophysiologic Monitoring: Basic Principles and Recent Update
- Monitoring of Somatosensory Evoked Potentials During Intracranial Aneurysm Surgery
- A New Measure for Monitoring Intraoperative Somatosensory Evoked Potentials
- Cerebral somatosensory evoked potentials in children with cerebral palsy
