Distal Fibular Rotational Plasty for Chronic Peroneal Tendon Recurrent Dislocation: A Technical Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Dankook University College of Medicine, Cheonan, Korea
- KMID: 2509540
- DOI: http://doi.org/10.14193/jkfas.2020.24.4.168
Abstract
- Chronic recurrent peroneal dislocation often responds poorly to conservative treatment. Surgical treatment has been reported to be more effective than conservative treatment, and various surgical treatment methods are available: superior peroneal retinaculum repair or reattachment, peroneal groove deepening procedures, rerouting procedures, or bone block procedures. Although various treatment options have been reported, there is no consensus regarding which treatment is better. This paper proposes a distal fibular rotational plasty that can prevent recurrent peroneal dislocations and recover its function well by securing a stable peroneal tendon excursion space.
Keyword
Figure
-

Fig. 1 Operative technique. (A) After the longitudinal incision posterolateral to the distal fibular, the peroneal tendon sheath and superior peroneal retinaculum (SPR) were incised leaving a 3-mm cuff at the posterior border of the fibula and then, the dislocated peroneal tendon was observed. Black arrow heads indicate dislocated peroneus longus. (B) After dislocating the peroneal brevis and longus tendon laterally (asterisk [*] indicates fibrocartilaginous ridge), (C) the osteotomy with sagittal saw was done 3 cm proximally to the distal tip of the fibula from posterolateral margin of the peroneal groove with 5 mm in depth to the half width of the distal fibular. In this process, the fibrocartilaginous surface of peroneal groove was preserved as much as possible by including the fibrocartilaginous ridge and cutting at just posterolateral margin of the peroneal groove. (D) The bone block was temporary fixed with two K-wires after rotating 15~20 degrees counterclockwise and making 5 mm roof to preventing tendon dislocation at posterolateral aspect of distal tip of fibula. The C-arm fluoroscopy image showed the direction of K-wires. The proximal K-wire was inserted vertically, and the distal one was inserted with oblique direction from posterolateral bone block to anteromedial distal fibula. (E) The bone block was fixed with two 4.0 mm cancellous screws along the direction of the K-wires. (F) The peroneal brevis and longus tendon were relocated and the stability of tendon was confirmed with a stress test. The firm screw fixation and no penetration of screws to the joint were confirmed with the C-arm fluoroscopy. (G) The SPR was repaired to the posterolateral margin of the fibula without damage to a fibrocartilaginous ridge and the fascia was closed. And the stability of tendon was confirmed again with a stress test and the skin repaired layer by layer (asterisk [*] indicates fibrocartilaginous ridge).

Fig. 2 The illustration shows distal fibular rotational plasty in the lateral view of the ankle. The black arrow shows a fibrocartilaginous ridge.
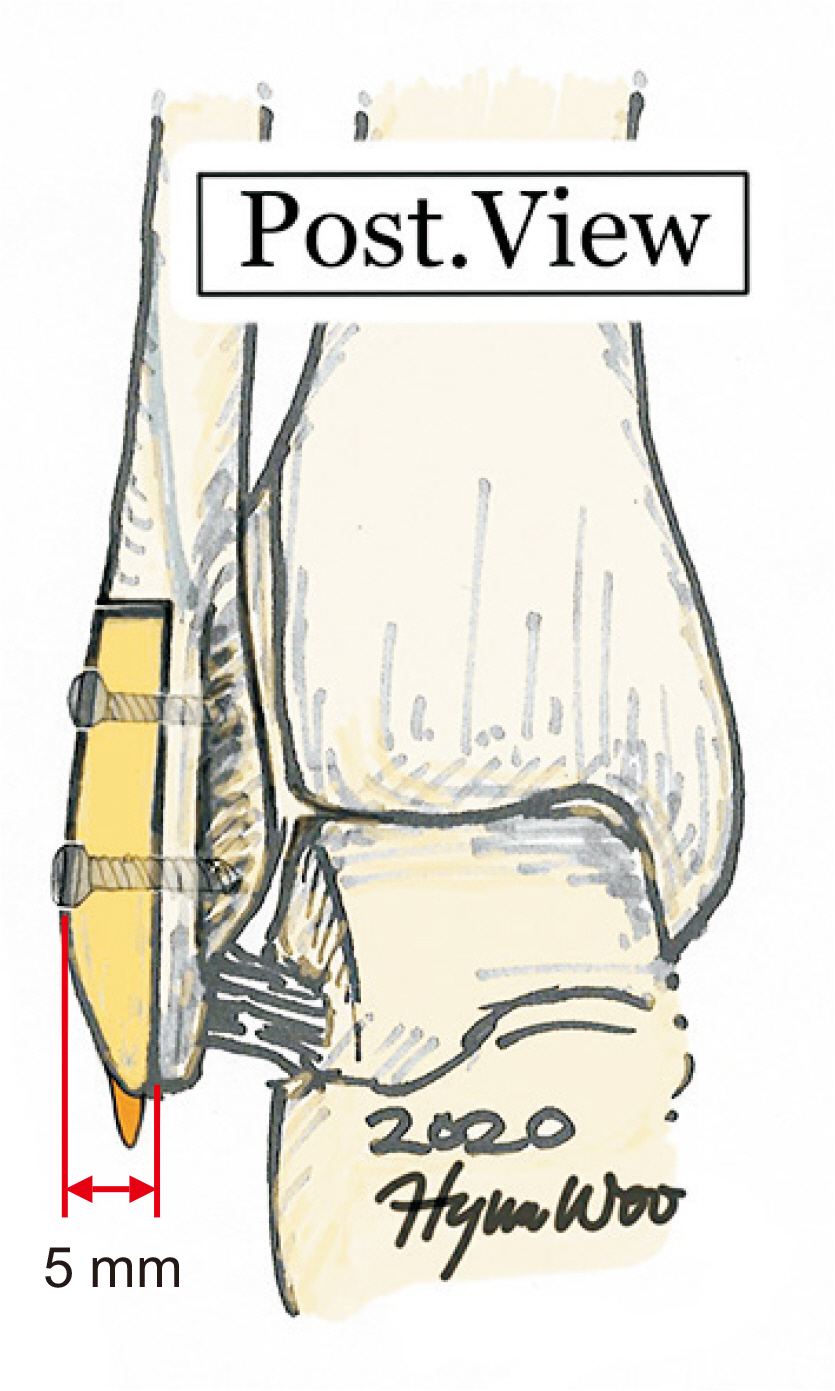
Fig. 3 The illustration of the operative technique shows a posterior view of the ankle. It shows the osteotomy line at just the posterolateral margin of the peroneal groove, and the bone block, including the fibrocartilaginous ridge, is made in 5 mm-depth.
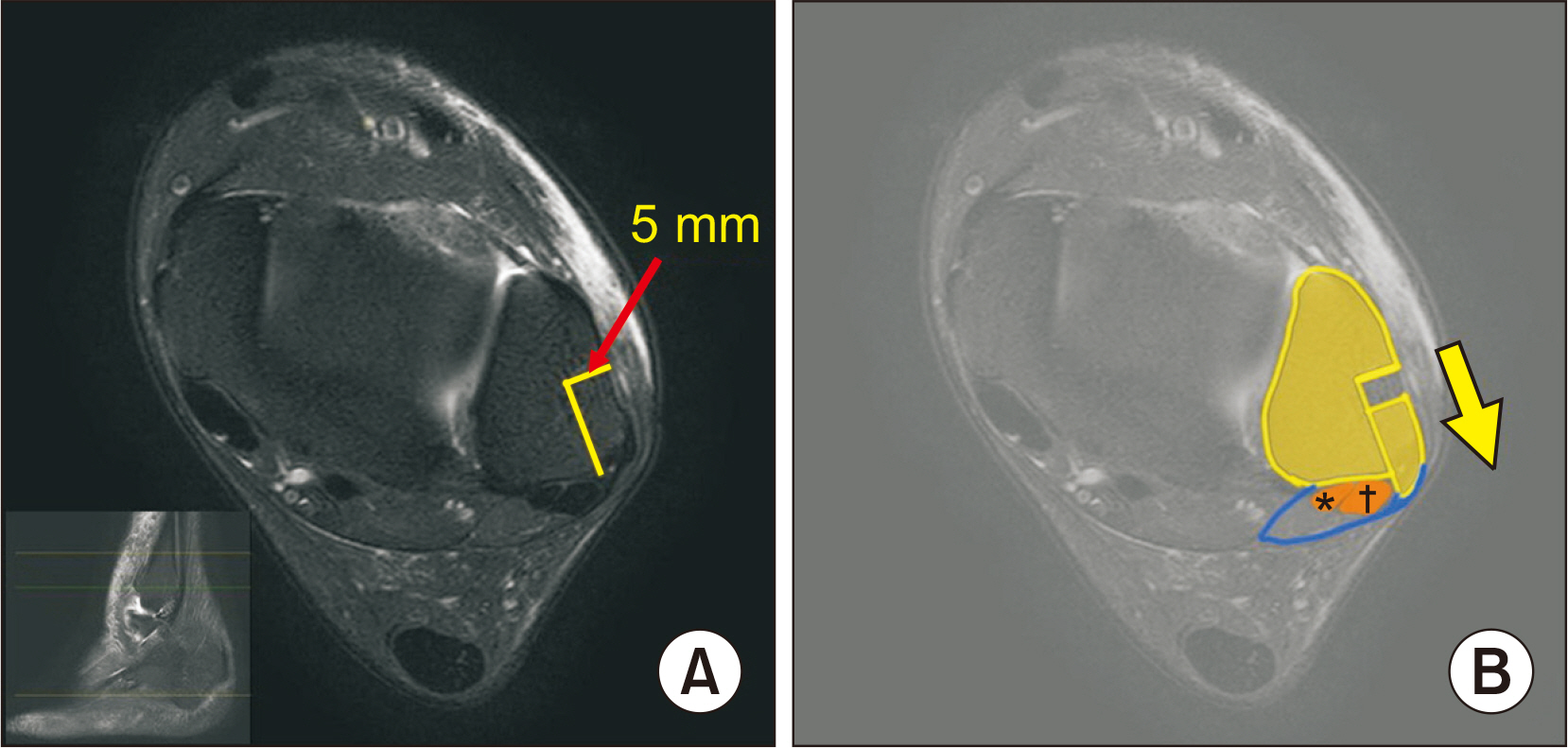
Fig. 4 The axial image of magnetic resonance imaging (MRI) with the illustration shows the concept of distal fibular rotational plasty. With 5 mm depth bone block (A), the roof is made to prevent tendon dislocation and to restore enough volume of the peroneal tendon excursion space (B). *Peroneus brevis. †Peroneus longus.

Fig. 5 The illustration of the operative technique shows a posterolateral view of the ankle. It shows a 5 mm-width roof to prevent tendon dislocation at the posterolateral aspect of the distal fibular tip.
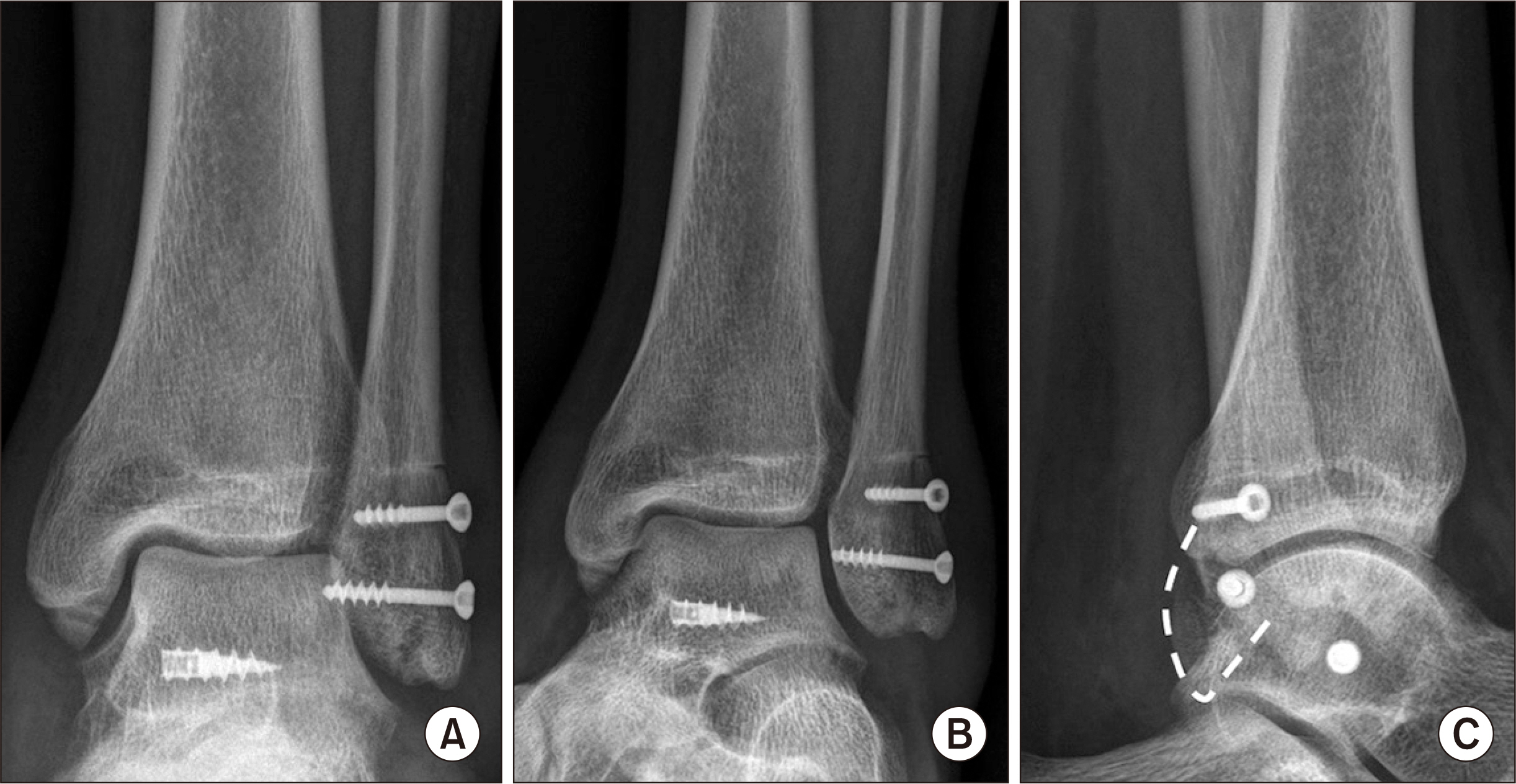
Fig. 6 Postoperative anteroposterior (A), mortise (B), and lateral (C) ankle radiographs of a 29-year-old male patient who had chronic recurrent peroneal dislocation and medial ankle instability at 10 weeks after surgery. These show successful bone union without any penetration of the two cancellous screws to the ankle joint. (C) The white dotted line shows a rotated bone block roof.
Reference
-
1. van Dijk PAD, Vopat BG, Guss D, Younger A, DiGiovanni CW. 2017; Retromalleolar groove deepening in recurrent peroneal tendon dislocation: technique tip. Orthop J Sports Med. 5:2325967117706670. doi: 10.1177/2325967117706673. DOI: 10.1177/2325967117706673. PMID: 28540318. PMCID: PMC5431455.
Article2. Suh JW, Lee JW, Park JY, Choi WJ, Han SH. 2018; Posterior fibular groove deepening procedure with low-profile screw fixation of fibrocartilaginous flap for chronic peroneal tendon dislocation. J Foot Ankle Surg. 57:478–83. doi: 10.1053/j.jfas.2017.10.033. DOI: 10.1053/j.jfas.2017.10.033. PMID: 29269024.
Article3. Cho J, Kim JY, Song DG, Lee WC. 2014; Comparison of outcome after retinaculum repair with and without fibular groove deepening for recurrent dislocation of the peroneal tendons. Foot Ankle Int. 35:683–9. doi: 10.1177/1071100714531233. DOI: 10.1177/1071100714531233. PMID: 24709746.
Article4. Heckman DS, Reddy S, Pedowitz D, Wapner KL, Parekh SG. 2008; Operative treatment for peroneal tendon disorders. J Bone Joint Surg Am. 90:404–18. doi: 10.2106/JBJS.G.00965. DOI: 10.2106/JBJS.G.00965. PMID: 18245603.
Article5. van Dijk PA, Gianakos AL, Kerkhoffs GM, Kennedy JG. 2016; Return to sports and clinical outcomes in patients treated for peroneal tendon dislocation: a systematic review. Knee Surg Sports Traumatol Arthrosc. 24:1155–64. doi: 10.1007/s00167-015-3833-z. DOI: 10.1007/s00167-015-3833-z. PMID: 26519186. PMCID: PMC4823328.
Article6. Tomihara T, Shimada N, Yoshida G, Kaneda K, Matsuura T, Satake S. 2010; Comparison of modified Das De procedure with Du Vries procedure for traumatic peroneal tendon dislocation. Arch Orthop Trauma Surg. 130:1059–63. doi: 10.1007/s00402-010-1136-x. DOI: 10.1007/s00402-010-1136-x. PMID: 20556617.
Article7. Wang CC, Wang SJ, Lien SB, Lin LC. 2009; A new peroneal tendon rerouting method to treat recurrent dislocation of peroneal tendons. Am J Sports Med. 37:552–7. doi: 10.1177/0363546508325924. DOI: 10.1177/0363546508325924. PMID: 19059898.
Article8. Ogawa BK, Thordarson DB. 2007; Current concepts review: peroneal tendon subluxation and dislocation. Foot Ankle Int. 28:1034–40. doi: 10.3113/FAI.2007.1034. DOI: 10.3113/FAI.2007.1034. PMID: 17880883.9. Zhenbo Z, Jin W, Haifeng G, Huanting L, Feng C, Ming L. 2014; Sliding fibular graft repair for the treatment of recurrent peroneal subluxation. Foot Ankle Int. 35:496–503. doi: 10.1177/1071100714523271. DOI: 10.1177/1071100714523271. PMID: 24637656.
Article10. Deng E, Shi W, Jiao C, Xie X, Jiang D, Chen L, et al. 2019; Reattachment of the superior peroneal retinaculum versus the bone block procedure for the treatment of recurrent peroneal tendon dislocation: two safe and effective techniques. Knee Surg Sports Traumatol Arthrosc. 27:2877–83. doi: 10.1007/s00167-019-05479-2. DOI: 10.1007/s00167-019-05479-2. PMID: 30903219.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Operative Treatment for Bilateral Chronic Recurrent Dislocation of the Peroneal Tendon: A Case Report
- Operative Treatment of Chronic Recurrent Dislocation of Peroneal Tendon: A Case Report
- Bilateral Recurrent Dislocation of the Peroneal Tendon: A Case Report
- Treatment of Peroneal Tendon Subluxation by Fibular Groove Deepening
- Operative Treatment of Acute Peroneal Tendon Subluxation in Athletes: A Case Report - 2 Cases
