Feasibility of Posterior Cervical Foraminotomy for Adjacent Segmental Disease after Anterior Cervical Fusion
- Affiliations
-
- 1Department of Neurosurgery, Daegu Wooridul Spine Hospital, Daegu, Korea
- 2Department of Neurosurgery, Wooridul Spine Hospital, Seoul, Korea
- 3Department of Anesthesiology and Pain Medicine, Daegu Wooridul Spine Hospital, Daegu, Korea
- KMID: 2508607
- DOI: http://doi.org/10.3340/jkns.2020.0033
Abstract
Objective
: The aim of this study is to evaluate the feasibility of posterior cervical foraminotomy (PCF) for adjacent segmental disease (ASD) after anterior cervical fusion (ACF). As ACF is accepted as the standard treatment for cervical spondylosis, many studies have been conducted to evaluate the efficacy of various surgical techniques to overcome symptomatic ASD after the previous surgery. Herein, PCF was performed for the treatment of symptomatic ASD and the feasibility of the surgery was evaluated.
Methods
: Forty nine patients who underwent PCF due to symptomatic ASD from August 2008 to November 2017 were identified. For demographic and perioperative data, the sex, age, types of previous surgery, ASD levels, operation times, and bleeding amount were recorded. The clinical outcome was assessed using the visual analogue scale for the neck and arm, the modified Odom’s criteria as well as neck disability index. Radiologic evaluations were performed by measuring disc softness, disc height, the cervical 2–7 sagittal vertical axis, cervical cobb angle, and facet violation.
Results
: Thirty-seven patients were enrolled in this study. The patients were divided into two groups based on the location of the pathology; paracentral (group P) or foramina (group F). Both groups showed significant clinical improvement (p<0.05). The proportion of calcified disc and facet violations was significantly larger in group F (p<0.05). The minimal disc height decrease with mild improvement on sagittal alignment and cervical lordosis was radiologically measured without statistical significance in both groups (p>0.05).
Conclusion
: PCF showed satisfactory clinical and radiologic outcomes for both paracentral and foraminal pathologies of ASD after ACF. Complications related to anterior revision were also avoided. PCF can be considered a feasible and safe surgical option for ASD after ACF.
Figure
-
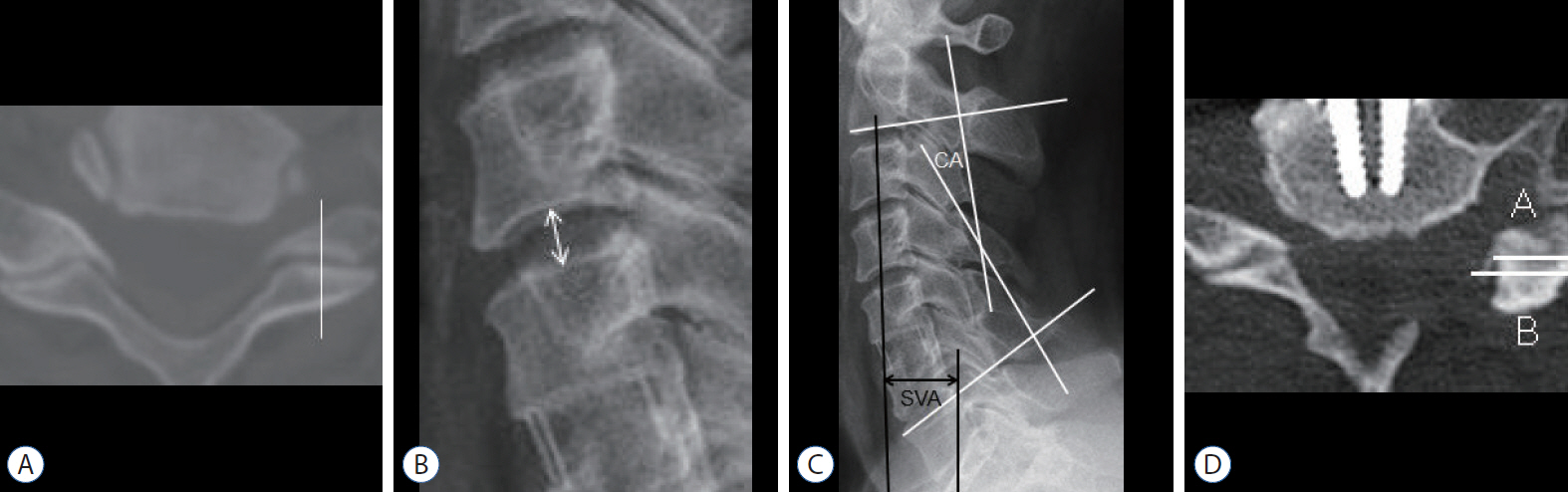
Fig. 1. A : The white line is the midline of the facet joint. Pathology across this line was categorized as paracentral while that outside the line was categorized as foraminal. B : Double headed arrow indicates the disc height. It was measured as the length from the midpoint of the upper endplate of the lower vertebral body to the midpoint of the lower endplate of the upper vertebral body. C : The C2–7 sagittal vertical axis (SVA) was measured as the length from the vertical line starting at the center of the C2 vertebral body (vertical black line) to the end point of the superior posterior of the C7 vertebral body (horizontal black line). The cervical Cobb angle (CA) was measured as the angle between two lines parallel to the lower margin of the C2 vertebral body and the upper margin of the C7 vertebral body (white lines). D : The amount of facet resection was measured as the proportion of resected facet (A, white line) compared to the original facet (B, white line). The formula was (A–B) / A × 100.

Fig. 2. A : Disc height change with time shows a minimal decrease after posterior cervical foraminotomy (PCF). B : C2–7 sagittal vertical axis change with time shows the improvement of the sagittal alignment after PCF. C : Cervical Cobb angle with time shows mild recovery of cervical lordosis after PCF. Pre-op : preoperation, Post-op : postoperation, f/u : follow up.
Reference
-
References
1. Basques BA, Ondeck NT, Geiger EJ, Samuel AM, Lukasiewicz AM, Webb ML, et al. Differences in short-term outcomes between primary and revision anterior cervical discectomy and fusion. Spine (Phila Pa 1976). 42:253–260. 2017.
Article2. Bayoumi AB, Berk S, Efe IE, Bas EG, Duran M, Yigit T, et al. Posterior cervical keyhole laminoforaminotomy: a cadaveric comparative study to evaluate limits of bony resection. Oper Neurosurg (Hagerstown). 16:607–613. 2019.
Article3. Bydon M, Xu R, De la Garza-Ramos R, Macki M, Sciubba DM, Wolinsky JP, et al. Adjacent segment disease after anterior cervical discectomy and fusion: incidence and clinical outcomes of patients requiring anterior versus posterior repeat cervical fusion. Surg Neurol Int. 5(Suppl 3):S74–S78. 2014.
Article4. Cho TG, Kim YB, Park SW. Long term effect on adjacent segment motion after posterior cervical foraminotomy. Korean J Spine. 11:1–6. 2014.
Article5. Chung SW, Kim HJ, Lee SH, Lee SY, Kang MS, Shin YH, et al. Posterior cervical foraminotomy for cervical radiculopathy: should cervical alignment be considered? J Spine Surg. 5:541–548. 2019.
Article6. Gu BS, Park JH, Seong HY, Jung SK, Roh SW. Feasibility of posterior cervical foraminotomy in cervical foraminal stenosis: prediction of surgical outcomes by the foraminal shape on preoperative computed tomography. Spine (Phila Pa 1976). 42:E267–E271. 2017.7. Guo Q, Wang L, Zhang B, Jiang J, Guo X, Lu X, et al. Standalone anterior cervical discectomy and fusion versus combination with foraminotomy for the treatment of cervical spondylotic radiculopathy secondary to bony foraminal stenosis. World Neurosurg. 95:134–142. 2016.
Article8. Han SY, Kim HW, Lee CY, Kim HR, Park DH. Stand-alone cages for anterior cervical fusion: are there no problems? Korean J Spine. 13:13–19. 2016.
Article9. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH. Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am. 81:519–528. 1999.
Article10. Kang MS, Choi KC, Lee CD, Shin YH, Hur SM, Lee SH. Effective cervical decompression by the posterior cervical foraminotomy without discectomy. J Spinal Disord Tech. 27:271–276. 2014.
Article11. Kim KT, Cho DC, Sung JK, Kim YB, Kim DH. Comparative analysis between total disc replacement and posterior foraminotomy for posterolateral soft disc herniation with unilateral radiculopathy : clinical and biomechanical results of a minimum 5 years follow-up. J Korean Neurosurg Soc. 60:30–39. 2017.
Article12. Kim SJ, Seo JS, Lee SH, Bae J. Comparison of anterior cervical foraminotomy and posterior cervical foraminotomy for treating single level unilateral cervical radiculopathy. Spine (Phila Pa 1976). 44:1339–1347. 2019.
Article13. Kretzer RM, Hsu W, Hu N, Umekoji H, Jallo GI, McAfee PC, et al. Adjacent-level range of motion and intradiscal pressure after posterior cervical decompression and fixation: an in vitro human cadaveric model. Spine (Phila Pa 1976). 37:E778–E785. 2012.14. Lee SB, Cho KS. Cervical arthroplasty versus anterior cervical fusion for symptomatic adjacent segment disease after anterior cervical fusion surgery: review of treatment in 41 patients. Clin Neurol Neurosurg. 162:59–66. 2017.
Article15. Lee YS, Kim YB, Park SW, Kang DH. Preservation of Motion at the Surgical Level after Minimally Invasive Posterior Cervical Foraminotomy. J Korean Neurosurg Soc. 60:433–440. 2017.
Article16. Li J, Tong T, Niu R, Shen Y. A study on the clinical outcomes of patients with revision surgery for adjacent segment disease after 10-year's anterior cervical spine surgery. J Orthop Surg Res. 11:5. 2016.
Article17. Lin GX, Rui G, Sharma S, Kotheeranurak V, Suen TK, Kim JS. Does the neck pain, function, or range of motion differ after anterior cervical fusion, cervical disc replacement, and posterior cervical foraminotomy? World Neurosurg. 129:e485–e493. 2019.
Article18. Lu VM, Mobbs RJ, Phan K. Clinical outcomes of treating cervical adjacent segment disease by anterior cervical discectomy and fusion versus total disc replacement: a systematic review and meta-analysis. Global Spine J. 9:559–567. 2019.
Article19. Lubelski D, Healy AT, Silverstein MP, Abdullah KG, Thompson NR, Riew KD, et al. Reoperation rates after anterior cervical discectomy and fusion versus posterior cervical foraminotomy: a propensity-matched analysis. Spine J. 15:1277–1283. 2015.
Article20. Ryan J, McGowan JE, Voyadzis JM. Treating cervical radiculopathy for a one-level disc herniation using a posterior foraminotomy. Semin Spine Surg. 26:148–153. 2014.
Article21. van Eck CF, Regan C, Donaldson WF, Kang JD, Lee JY. The revision rate and occurrence of adjacent segment disease after anterior cervical discectomy and fusion: a study of 672 consecutive patients. Spine (Phila Pa 1976). 39:2143–2147. 2014.
Article22. Wang F, Wang P, Miao DC, Du W, Shen Y. Different surgical approaches for the treatment of adjacent segment diseases after anterior cervical fusion: a retrospective study of 49 patients. Medicine (Baltimore). 96:e7042. 2017.23. Zdeblick TA, Zou D, Warden KE, McCabe R, Kunz D, Vanderby R. Cervical stability after foraminotomy. A biomechanical in vitro analysis. J Bone Joint Surg Am. 74:22–27. 1992.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Long Term Effect on Adjacent Segment Motion after Posterior Cervical Foraminotomy
- Posterior Endoscopic Cervical Discectomy
- Fully-Endoscopic Posterior Cervical 2-Level Foraminotomy With Total Pediculectomy for Adjacent-Level Foraminal Stenosis in Severe Degenerative Spondylolisthesis: A Technical Note With 1-Year Follow-up
- Clinical Results of Microsurgical Anterior Foraminotomy for Cervical Radiculopathy
- Application of Posterior Endoscopic Cervical Foraminotomy for Recurrent Radiculopathy After Anterior Cervical Discectomy and Fusion Surgery
