Rotablator Driveshaft Fracture Due to Significant Proximal Tortuosity and Enlargement Causing Massive Coronary Perforation
- Affiliations
-
- 1Department of Cardiovascular Medicine, Sapporo Cardio Vascular Clinic, Sapporo Heart Center, Sapporo, Japan
- KMID: 2508282
- DOI: http://doi.org/10.4070/kcj.2020.0136
Figure
-
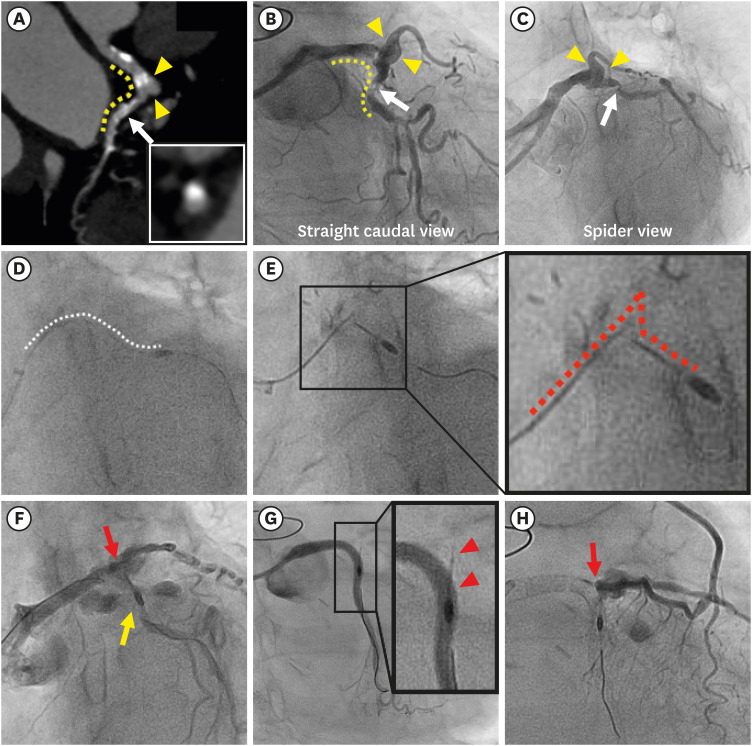
Figure 1 Computed tomographic, fluoroscopic and angiographic images. (A-C) Baseline computed tomography and coronary angiography revealing severe tortuosity (yellow dotted line) and enlargement (yellow arrowheads) proximal to the culprit lesion (white arrow). The inset in A demonstrated a protruding calcified nodule. (D) The white dotted line indicates the normal course of the driveshaft during initial rotablation. (E) Prolapse and fracture of the driveshaft (red dotted line) at the extremely tortuous and enlarged segment. The inset presents an enlarged image. (F) Ellis type III coronary perforation of the distal left main with vascular ectasia (red allow) and left circumflex artery (yellow allow). (G) Left coronary angiography showing no contrast extravasation. The inset presents an enlarged image of the fractured and remnant driveshaft (red arrowheads). (H) Persistent contrast extravasation confirmed by angiography of left internal mammary artery to left anterior descending artery graft (red arrow).

Figure 2 Computed tomographic, angiographic, and intravascular ultrasound images of rotational atherectomy using a 5Fr child guide catheter (“mother-and-child” technique). (A) Baseline CT showing heavily calcified chronic total occlusion lesion in the distal right coronary artery (white arrow). The inset shows a cross-sectional CT image of the culprit lesion with dense calcification. (B, C) Baseline coronary angiography (B: LAO cranial view, C: RAO view) revealing severe tortuosity (yellow dotted line) proximal to the culprit lesion (white arrow). (D) Deep insertion of 5Fr child guide catheter (Heartrail ST01, Terumo, Tokyo, Japan) (yellow arrow) beyond the tortuous segment, by the anchor balloon technique. (Inset in D) After predilatation with 2.25-mm semicompliant balloon resulted in underexpansion, intravascular ultrasound images of the distal RCA lesion (white arrow) revealed severe concentric calcification. (E) Deep insertion of the child guide catheter (yellow arrow) beyond the tortuous segment enabled smooth delivery of a 1.25-mm burr (red arrow) and rotational atherectomy. (F) Final angiography after stenting and postdilatation. White line indicates the implanted stent.CT = computed tomography; LAO = left anterior oblique; RAO = right anterior oblique.
Reference
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Study of Branching Anomaly and Tortuosity of Radial Artery for Trans-Radial Coronary Procedure
- Spontaneous Perforation of Small Bowel Lymphoma Causing Massive Pneumoperitoneum: A case Report
- Guidewire-Induced Perforation of Distal Circumflex Artery Treated with Transcatheter Embolization of Polyvinyl Alcohol Form
- Clinical Aspects of Coronary Artery Perforation during Percutaneous Coronary Intervention
- Coronary Stent Fracture in a Patient with an Atrial Septal Defect and Severe Pulmonary Hypertension
