Pediatric split liver transplantation using a hyperreduced left lateral segment graft in an infant weighing 4 kg
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Department of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2507166
- DOI: http://doi.org/10.4285/kjt.2020.34.3.204
Abstract
- We present a case of successful split liver transplantation (LT) using a hyperreduced left lateral segment (LLS) graft in a 106-day-old female infant patient weighing 4 kg. The patient was diagnosed with progressive familial intrahepatic cholestasis. Her general condition and liver function deteriorated progressively and she was finally allocated for a split LT under status 1. The deceased donor was a 20-year-old female weighing 63.7 kg. We performed in situ liver splitting and in situ size reduction sequentially. The weight of the hyperreduced LLS graft was 225 g, with a graft-recipient weight ratio of 5.5%. We performed recipient hepatectomy and graft implantation according to the standard procedures for pediatric living-donor LT. Since the graft was too large for primary abdomen closure, the abdominal wall was closed in three stages to make a prosthetic silo, temporary closure with a xenograft sheet, and final primary repair over 2 weeks. The patient has been doing well for more than 6 years after transplantation. In conclusion, split LT using a hyperreduced LLS graft can be a useful option for treating small infants. However, large-for-size graft-related problems, particularly in terms of graft thickness, still remain to be solved.
Keyword
Figure
-

Fig. 1 Pretransplant computed tomography (CT) and explant liver findings. (A) CT scan taken 2 months after birth showed marked hepatomegaly and liver cirrhosis. (B) The explant liver showed a mixed type of macronodular and micronodular cirrhosis.

Fig. 2 Recovery of the hyperreduced left lateral segment graft through in situ splitting and in situ reduction. (A) The lines for in situ splitting and size reduction were marked at the surface of the donor liver. (B) In situ size reduction was carried out without a Pringle maneuver. (C) Liver splitting and size reduction were completed. (D) The split liver grafts were divided at the back table in the operating room.
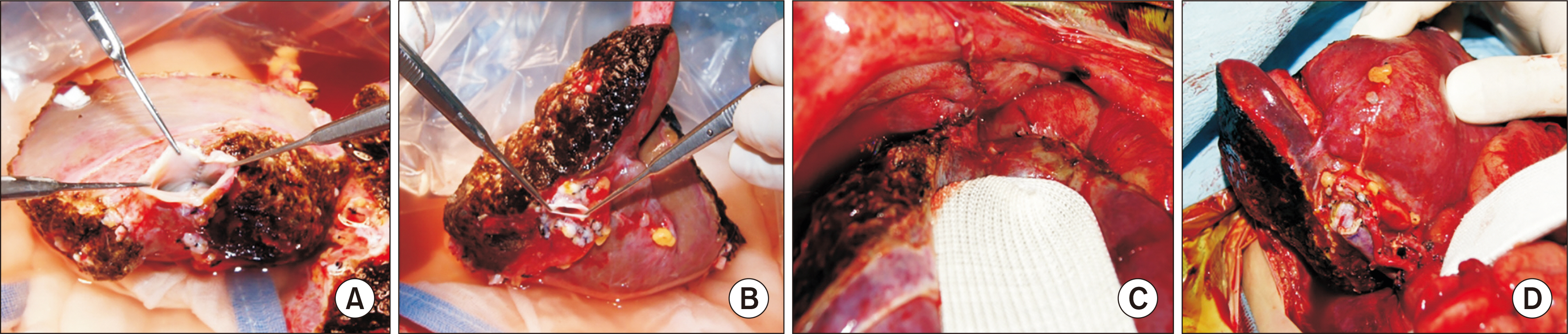
Fig. 3 Graft preparation and vascular reconstruction. (A) The graft hepatic vein branches were unified through unification venoplasty after septotomy and excision of the intervening hepatic parenchyma. (B) The size of the graft portal vein was measured. (C) The hepatic vein orifice of the graft was anastomosed to the unified hepatic vein openings at the inferior vena cava. (D) Portal vein reconstruction was carried out using a branch patch of the recipient’s portal vein and one left hepatic artery was reconstructed under surgical microscopy.
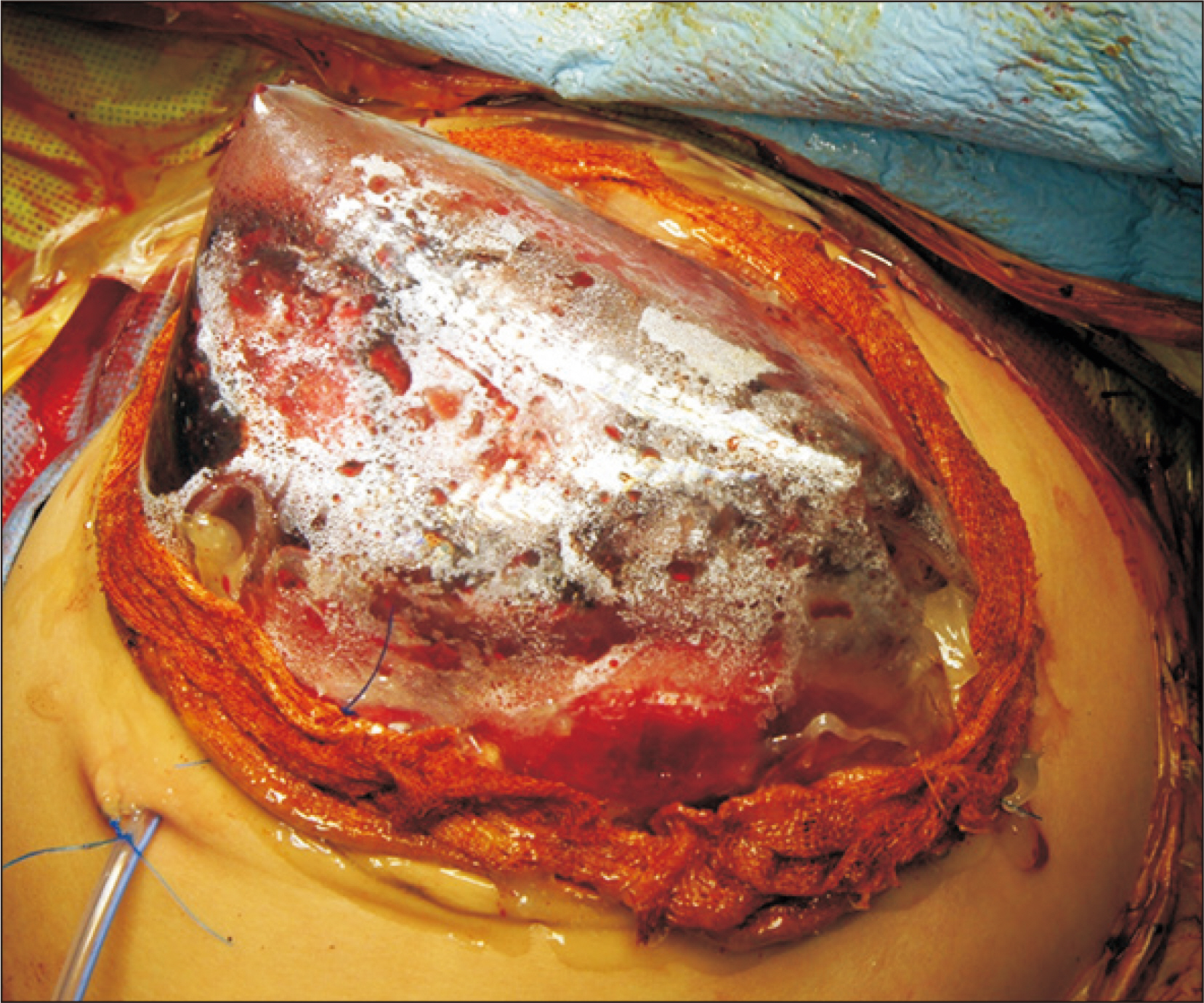
Fig. 4 Temporary abdominal wall closure. A silo using a transparent prosthetic sheet was attached to cover the liver graft as the liver graft bulged out through the abdominal incision.

Fig. 5 Computed tomography scan taken four days after transplantation. There was an abdominal wall defect (A, B) but the configurations of the hepatic vein (C) and portal vein (D) reconstruction were both smoothly streamlined.

Fig. 6 Computed tomography scan taken 14 days after transplantation. The abdominal wall was closed completely (A, B) and the graft hepatic vein (C) and portal vein (D) reconstructions were uneventful.
Cited by 3 articles
-
Dextroplantation of a reduced left lateral section graft in an infant undergoing living donor liver transplantation
Jung-Man Namgoong, Shin Hwang, Gil-Chun Park, Kyung Mo Kim, Seak Hee Oh, Hyunhee Kwon, Yong Jae Kwon
Ann Hepatobiliary Pancreat Surg. 2021;25(3):414-418. doi: 10.14701/ahbps.2021.25.3.414.Pediatric deceased donor liver transplantation with
in situ size reduction for recipient-graft size matching
Jung-Man Namgoong, Shin Hwang, Dae-Yeon Kim, Tae-Yong Ha, Gi-Won Song, Dong-Hwan Jung, Kyung Mo Kim, Seak Hee Oh
Ann Hepatobiliary Pancreat Surg. 2021;25(3):431-435. doi: 10.14701/ahbps.2021.25.3.431.Living donor liver transplantation with hyperreduced segment II monosegment graft for an infant weighing 3 kilograms
Jung-Man Namgoong, Gil-Chun Park, Shin Hwang, Sang-Hoon Kim, Suhyeon Ha, Kyung Mo Kim, Seak Hee Oh
Ann Liver Transplant. 2023;3(1):50-56. doi: 10.52604/alt.23.0001.
Reference
-
1. Kanazawa H, Sakamoto S, Fukuda A, Uchida H, Hamano I, Shigeta T, et al. 2013; Living-donor liver transplantation with hyperreduced left lateral segment grafts: a single-center experience. Transplantation. 95:750–4. DOI: 10.1097/TP.0b013e31827a93b4. PMID: 23503505.2. Shehata MR, Yagi S, Okamura Y, Iida T, Hori T, Yoshizawa A, et al. 2012; Pediatric liver transplantation using reduced and hyper-reduced left lateral segment grafts: a 10-year single-center experience. Am J Transplant. 12:3406–13. DOI: 10.1111/j.1600-6143.2012.04268.x. PMID: 22994696.
Article3. Ardiles V, Ciardullo MA, D'Agostino D, Pekolj J, Mattera FJ, Boldrini GH, et al. 2013; Transplantation with hyper-reduced liver grafts in children under 10 kg of weight. Langenbecks Arch Surg. 398:79–85. DOI: 10.1007/s00423-012-1020-y. PMID: 23093088.4. Thomas N, Thomas G, Verran D, Stormon M, O'Loughlin E, Shun A. 2010; Liver transplantation in children with hyper-reduced grafts: a single-center experience. Pediatr Transplant. 14:426–30. DOI: 10.1111/j.1399-3046.2010.01294.x. PMID: 20214746.5. Yamada N, Sanada Y, Hirata Y, Okada N, Wakiya T, Ihara Y, et al. 2015; Selection of living donor liver grafts for patients weighing 6kg or less. Liver Transpl. 21:233–8. DOI: 10.1002/lt.24048. PMID: 25422258.
Article6. Sakuma Y, Sasanuma H, Miki A, Shimizu A, Sata N, Yasuda Y, et al. 2016; Living-donor liver transplantation using segment 2 monosegment graft: a single-center experience. Transplant Proc. 48:1110–4. DOI: 10.1016/j.transproceed.2015.12.119. PMID: 27320568.
Article7. Hong SK, Suh KS, Kim HS, Yoon KC, Ahn SW, Kim H, et al. 2018; Pediatric living donor liver transplantation using a monosegment procured by pure 3D laparoscopic left lateral sectionectomy and in situ reduction. J Gastrointest Surg. 22:1135–6. DOI: 10.1007/s11605-018-3705-1. PMID: 29435902.
Article8. Srinivasan P, Vilca-Melendez H, Muiesan P, Prachalias A, Heaton ND, Rela M. 1999; Liver transplantation with monosegments. Surgery. 126:10–2. DOI: 10.1067/msy.1999.98686. PMID: 10418586.
Article9. Kiuchi T, Kasahara M, Uryuhara K, Inomata Y, Uemoto S, Asonuma K, et al. 1999; Impact of graft size mismatching on graft prognosis in liver transplantation from living donors. Transplantation. 67:321–7. DOI: 10.1097/00007890-199901270-00024. PMID: 10075602.10. Kasahara M, Fukuda A, Yokoyama S, Sato S, Tanaka H, Kuroda T, et al. 2008; Living donor liver transplantation with hyperreduced left lateral segments. J Pediatr Surg. 43:1575–8. DOI: 10.1016/j.jpedsurg.2008.02.056. PMID: 18675660.
Article11. Vanatta JM, Esquivel CO. 2007; Status of liver transplantation in infants < 5 kg. Pediatr Transplant. 11:5–9. DOI: 10.1111/j.1399-3046.2006.00627.x. PMID: 17328158.12. Raices M, Czerwonko ME, Ardiles V, Boldrini G, D'Agostino D, Marcó Del Pont J, et al. 2019; Short- and long-term outcomes after live-donor transplantation with hyper-reduced liver grafts in low-weight pediatric recipients. J Gastrointest Surg. 23:2411–20. DOI: 10.1007/s11605-019-04188-y. PMID: 30887299.
Article13. Houssin D, Soubrane O, Boillot O, Dousset B, Ozier Y, Devictor D, et al. 1992; Orthotopic liver transplantation with a reduced-size graft: an ideal compromise in pediatrics? Surgery. 111:532–42. PMID: 1598673.14. Sakamoto S, Kanazawa H, Shigeta T, Uchida H, Sasaki K, Hamano I, et al. 2014; Technical considerations of living donor hepatectomy of segment 2 grafts for infants. Surgery. 156:1232–7. DOI: 10.1016/j.surg.2014.05.003. PMID: 24909347.
Article15. Hwang S, Kim KH, Kim DY, Kim KM, Ahn CS, Moon DB, et al. 2013; Anomalous hepatic vein anatomy of left lateral section grafts and customized unification venoplasty for pediatric living donor liver transplantation. Liver Transpl. 19:184–90. DOI: 10.1002/lt.23557. PMID: 23045153.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Living donor liver transplantation with hyperreduced segment II monosegment graft for an infant weighing 3 kilograms
- Pediatric liver transplantation with hyperreduced left lateral segment graft
- Pediatric liver transplantation with hyperreduced left lateral segment graft
- Dextroplantation of a reduced left lateral section graft in an infant undergoing living donor liver transplantation
- Left at right heterotopic implantation of left liver graft in adult-to-adult living donor liver transplantation: the technical concern for decision-making
