Microsurgical treatment for the recurrent cerebral aneurysm initially treated using coil embolization
- Affiliations
-
- 1Department of Neurosurgery, Busan Paik Hospital, Inje University School of Medicine, Busan, Korea
- 2Department of Radiology, Busan Paik Hospital, Inje University School of Medicine, Busan, Korea
- 3Department of Endocrinology, Haeundae Paik Hospital, Inje University School of Medicine, Busan, Korea
- KMID: 2506763
- DOI: http://doi.org/10.7461/jcen.2020.22.3.165
Abstract
Objective
Microsurgical treatment could be a good alternative for the treatment of recurrent cerebral aneurysm after coil embolization. The purpose of this study was to present our experience of microsurgical treatment for recurrent cerebral aneurysm previously treated using coil embolization.
Methods
From June 2012 to May 2019, 34 patients consecutively received microsurgical treatment for a recurrent cerebral aneurysm previously treated using coil embolization after it ruptured.
Results
Of the 34 patients with aneurysm, 33 had the aneurysm located in the anterior circulation. The most common location was the anterior communicating artery (13 cases). Immediate radiologic outcome at coil embolization was completed (n=6), residual neck (n=26), and residual sac (n=2). The reason for microsurgical treatment included rebleeding (n=12), persistent residual sac (n=1), and recurrence on follow-up study (n=21). Rebleeding occurred within 10 days after coil embolization in 10 cases, and the other 2 were due to regrowth. In the 20 recurred and saccular aneurysms, coil compaction was present in 11 aneurysms and regrowth in 9 aneurysms. Simple neck clipping (n=29) and clipping with coil mass extraction (n=3) was possible in the saccular aneurysms. The blood blister like aneurysm (n=2) were treated using bypass and endovascular internal carotid artery trapping. In the follow-up study group after microsurgical treatment there were no severe complications due to the treatment. Age, cause of retreatment, and modified Rankin Scale before microsurgery were associated with good outcome (p<0.001).
Conclusions
Microsurgical treatment may be a viable and effective option for treating recurrent aneurysms previously treated by endovascular techniques.
Keyword
Figure
-

Fig. 1 (A) Drawing of a recurrent aneurysm that has a coil mass placed in the aneurysm dome (Dome type). Solid arrow indicates the neck. (B) Drawing of a recurrent aneurysm that has a coil mass placed in the neck of the aneurysm (Neck type). Solid arrow indicates the neck size and dotted arrow indicates the height of the aneurysm.

Fig. 2 Case 3, a 77-year-old male patient had a ruptured, partially thrombosed, left distal anterior cerebral artery (ACA) aneurysm. (A) A round mass was identified by a brain computed tomography (CT) scan. The mass was surrounded by subarachnoid hemorrhage and brain edema. (B) An aneurysm affecting some branching arteries of the neck was identified in left internal carotid artery (ICA) angiography; endosacular coiling was performed saving the branches at an outside hospital. (C) 7 months after coiling, rebleeding occurred. (D) Coil compaction and recanalization of the aneurysm were detected in left ICA Angiography. (E) Thrombi mixed with coils were extracted from the aneurysm. (F) Clips were securely placed, thrombi were removed, and aneurysmorrhaphy was performed. (G) Follow-up brain CT scan 1 month after microsurgery revealed reduced mass effect.
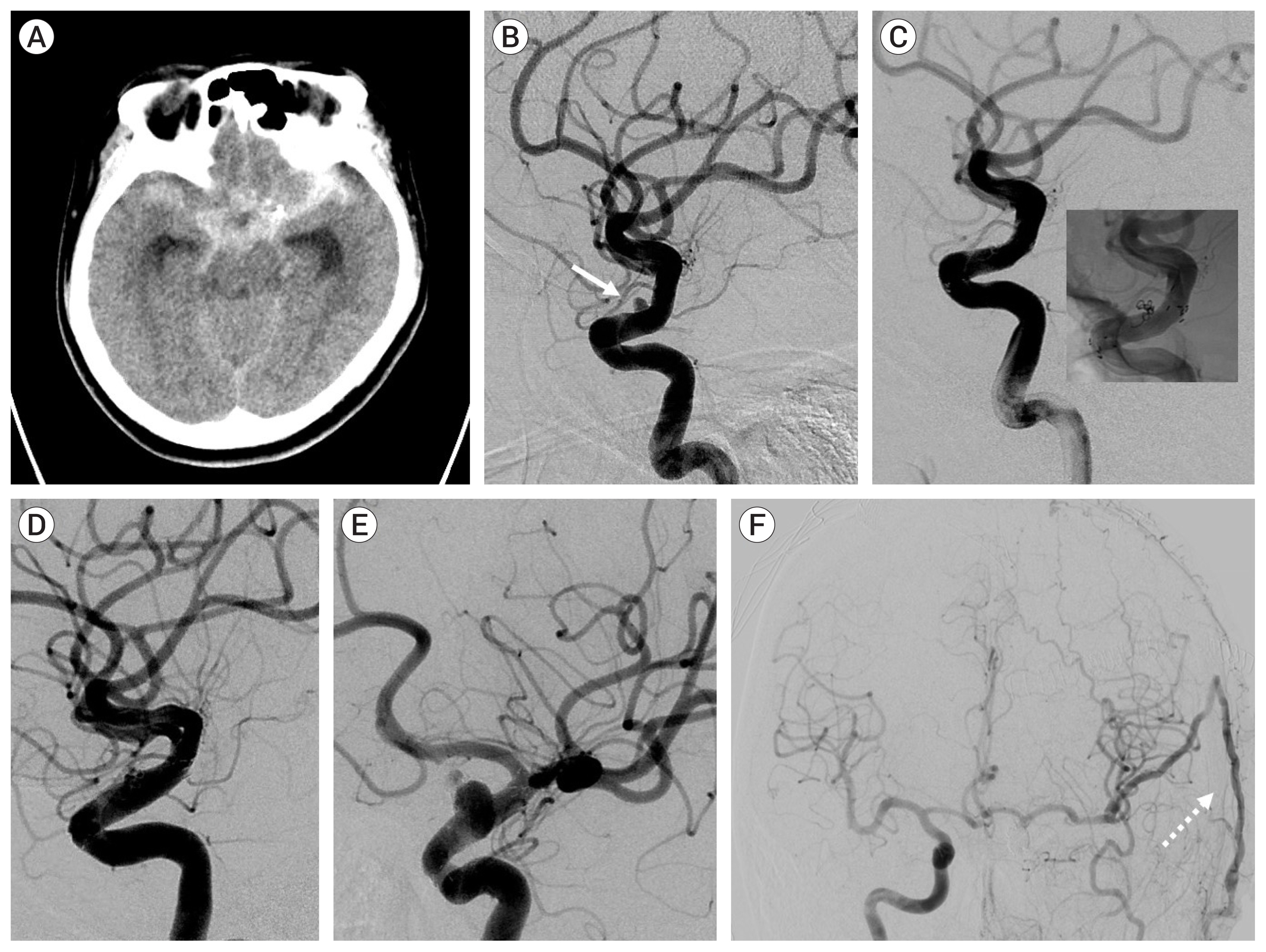
Fig. 3 Case 14, a 47-year-old female patient had a ruptured distal internal carotid artery (ICA) blood blister like aneurysm (BBL). (A) Brain computed tomography scan reveals thick subarachnoid hemorrhage around the basal cistern. (B) Angiogram reveals left distal ICA BBL aneurysm (white arrow). (C) Coil packing and multiple stenting was performed and intrasaccular thrombosis progressed well after the procedure. (D) Pathological change at the BBL was detected at follow-up angiogram after 1 month. (E) Fusiform dilatation had progressed at 3-month angiogram. (F) ICA trapping using coils promoted collateral blood flow through the anterior communicating artery and the superficial temporal artery-radial artery-M2 short interposition bypass (white dotted arrow).

Fig. 4 Case 17, a 35-year-old male patient had a ruptured 4.1-mm sized anterior communicating artery aneurysm. (A) Rebleeding was identified by brain CT scan 1 week after coil embolization (black arrow). (B) Following rebleeding, there was no identifiable change of coil mesh (white arrow) at follow-up angiogram after rebleeding. (C) Intraoperative view of the anterior communicating artery aneurysm via the right pterional approach. We observed an inflow of blood to the dome of the aneurysm (white dotted arrow). (D) After being clipped, the aneurysm shrank, and the inflow of blood disappeared.
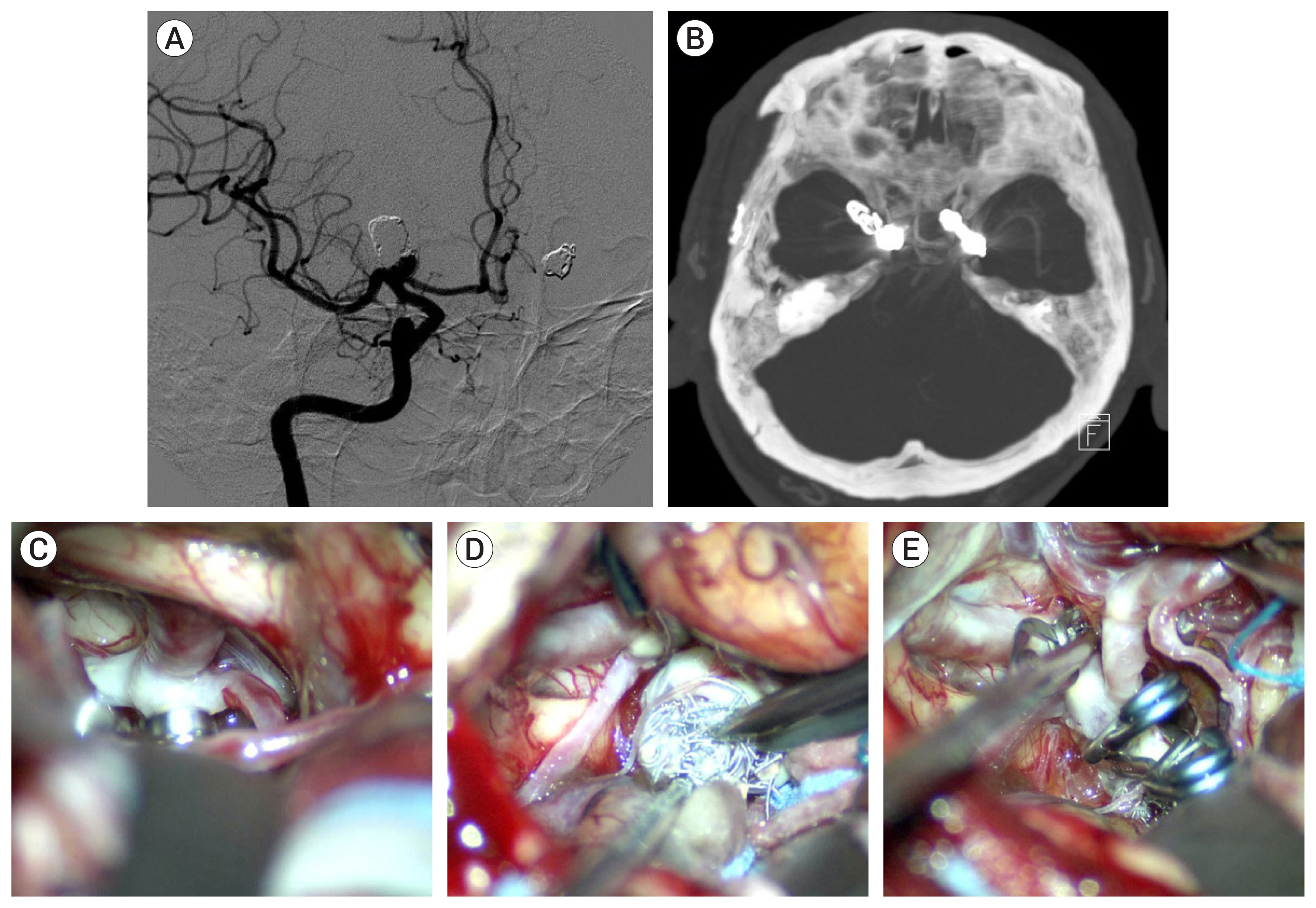
Fig. 5 Case 23, a 61-year-old male patient had recurring mirror aneurysms at both internal carotid artery bifurcations (ICAB) after coiling. Right side had previously ruptured. (A) Cerebral angiography revealed a neck type recurrence. (B) Clipping of both ICAB aneurysms was performed via right pterional approach. (C) At first, left ICAB aneurysm was secured by simple clipping. (D) There was severe adhesion between the right ICAB aneurysm and the surrounding tissue. Therefore, partial extraction of the coil mass partial was needed. (E) Using fenestration clip, neck clipping was possible. Unruptured posterior communicating artery aneurysm, not detected in cerebral angiography, was clipped together.
Cited by 1 articles
-
Microsurgical management of previously embolized intracranial aneurysms: A single center experience and literature review
Vasileios Panagiotopoulos, Ioannis Panagiotis Athinodorou, Kyprianos Kolios, Constantinos Kattou, Andreas Grzeczinski, Andreas Theofanopoulos, Lambros Messinis, Constantine Constantoyannis, Petros Zampakis
J Cerebrovasc Endovasc Neurosurg. 2025;27(1):1-18. doi: 10.7461/jcen.2024.E2024.05.004.
Reference
-
1. Ahn JY, Kim ST, Yi KC, Lee WH, Paeng SH, Jeong YG. Superficial temporal artery-sparing mini-pterional approach for cerebral aneurysm surgery. J Korean Neurosurg Soc. 2017; Jan. 60(1):8–14.
Article2. Arnaout OM, El Ahmadieh TY, Zammar SG, El Tecle NE, Hamade YJ, Aoun RJN, et al. Microsurgical treatment of previously coiled intracranial aneurysms: Systematic review of the literature. World Neurosurg. 2015; Aug. 84(2):246–53.
Article3. Bijlenga P, Morita A, Ko NU, Mocco J, Morel S, Murayama Y, et al. Common data elements for subarachnoid hemorrhage and unruptured intracranial aneurysms: Recommendations from the working group on subject characteristics. Neurocrit Care. 2019; Jun. 30(Suppl 1):20–27.
Article4. CARAT Investigators. Rates of delayed rebleeding from intracranial aneurysms are low after surgical and endovascular treatment. Stroke. 2006; Jun. 37(6):1437–42.5. Cho YD, Lee JY, Seo JH, Kang HS, Kim JE, Kwon OK, et al. Early recurrent hemorrhage after coil embolization in ruptured intracranial aneurysms. Neuroradiology. 2012; Jul. 54(7):719–26.
Article6. Dorfer C, Gruber A, Standhardt H, Bavinzski G, Knosp E. Management of residual and recurrent aneurysms after initial endovascular treatment. Neurosurgery. 2012; Mar. 70(3):537–53. discussion 553–4.
Article7. Izumo T, Matsuo T, Morofuji Y, Hiu T, Horie N, Hayashi K, et al. Microsurgical clipping for recurrent aneurysms after initial endovascular coil embolization. World Neurosurg. 2015; Feb. 83(2):211–8.
Article8. Johnston SC, Dowd CF, Higashida RT, Lawton MT, Duckwiler GR, Gress DR, et al. Predictors of rehemorrhage after treatment of ruptured intracranial aneurysms: The cerebral aneurysm rerupture after treatment (CARAT) study. Stroke. 2008; Jan. 39(1):120–5.9. Kim ST, Baek JW, Jin SC, Park JH, Kim JS, Kim HY, et al. Coil embolization in patients with recurrent cerebral aneurysms who previously underwent surgical clipping. AJNR Am J Neuroradiol. 2019; Jan. 40(1):116–21.
Article10. Kim ST, Baek JW, Lee WH, Lee KS, Kwon WH, Pyo S, et al. Causes of early rebleeding after coil embolization of ruptured cerebral aneurysms. Clin Neurol Neurosurg. 2018; Nov. 174:108–16.
Article11. Lawton MT, Lang MJ. The future of open vascular neurosurgery: Perspectives on cavernous malformations, AVMs, and bypasses for complex aneurysms. J Neurosurg. 2019; May. 130(5):1409–25.
Article12. Meling TR. What are the treatment options for blister-like aneurysms? Neurosurg Rev. 2017; Oct. 40(4):587–93.
Article13. Molyneux AJ, Birks J, Clarke A, Sneade M, Kerr RS. The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18 year follow-up of the UK cohort of the international subarachnoid aneurysm trial (ISAT). Lancet. 2015; Feb. 385(9969):691–7.
Article14. Murayama Y, Arakawa H, Ishibashi T, Kawamura D, Ebara M, Irie K, et al. Combined surgical and endovascular treatment of complex cerebrovascular diseases in the hybrid operating room. J Neurointerv Surg. 2013; Sep. 5(5):489–93.
Article15. Raymond J, Guilbert F, Weill A, Georganos SA, Juravsky L, Lambert A, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke. 2003; Jun. 34(6):1398–403.
Article16. Romani R, Lehto H, Laakso A, Horcajadas A, Kivisaari R, von und zu Fraunberg M, et al. Microsurgery for previously coiled aneurysms: Experience with 81 patients. Neurosurgery. 2011; Jan. 68(1):140–53. discussion 153–4.
Article17. Roy D, Milot G, Raymond J. Endovascular treatment of unruptured aneurysms. Stroke. 2001; Sep. 32(9):1998–2004.
Article18. Shtaya A, Dasgupta D, Millar J, Sparrow O, Bulters D, Duffill J. Outcomes of microsurgical clipping of recurrent aneurysms after endovascular coiling. World Neurosurg. 2018; Apr. 112:e540–7.
Article19. Spetzler RF, McDougall CG, Zabramski JM, Albuquerque FC, Hills NK, Nakaji P, et al. Ten-year analysis of saccular aneurysms in the barrow ruptured aneurysm trial. J Neurosurg. 2020; Mar. 132(3):771–6.
Article20. Toyota S, Kumagai T, Goto T, Mori K, Taki T. Clipping of recurrent cerebral aneurysms after coil embolization. Acta Neurochir Suppl. 2018; 129:53–9.
Article21. Waldron JS, Halbach VV, Lawton MT. Microsurgical management of incompletely coiled and recurrent aneurysms: Trends, techniques, and observations on coil extrusion. Neurosurgery. 2009; May. 64(5 Suppl 2):301–15. discussion 315–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Combined Endovascular and Microsurgical Procedures as Complementary Approaches in the Treatment of a Single Intracranial Aneurysm
- Endovascular Coil Embolization After Clipping: Endovascular Treatment of Incompletely Clipped or Recurred Cerebral Aneurysms
- Recent Trends in the Treatment of Cerebral Aneurysms: Comparison between Endovascular Coil Embolization and Surgical Clipping
- Coil Embolization for Distal Middle Cerebral Artery Aneurysm
- Microsurgical Clipping and Coil Removal of Previously Coiled Regrowing Cerebral Aneurysms
