Anesth Pain Med.
2020 Jul;15(3):365-370. 10.17085/apm.20020.
Does the minimal occlusive volume technique provide adequate endotracheal tube cuff pressure to prevent air leakage?: a prospective, randomized, crossover clinical study
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Dongguk University Ilsan Hospital, Goyang, Korea
- KMID: 2504900
- DOI: http://doi.org/10.17085/apm.20020
Abstract
- Background
Methods of determining proper endotracheal tube (ETT) cuff pressure to prevent air leakage include the minimal occlusive volume (MOV) technique, which uses auscultation, and the spirometer technique, which directly measures inspiratory and expiratory breathing volumes. Spirometers may measure even small air leakage, therefore, the spirometer technique requires a higher cuff pressure than the MOV technique to completely seal the airway. This study aimed to evaluate the difference in cuff pressure between the two techniques used to seal the airway.
Methods
Thirty-five female patients were intubated using an ETT with a cuff, and cuff inflation was performed with both techniques at a 10-min interval in random order—the MOV technique and then the spirometer technique or vice versa. The cuff pressure was measured at each period.
Results
The cuff pressures were 16.7 ± 1.2 cm H2O and 18.7 ± 1.3 cm H2O for the MOV and spirometer techniques, respectively. The cuff pressure for the spirometer technique was 2 cm H2O higher than that for the MOV technique and this difference was statistically significant (95% confidence interval, 0.7–3.3; P = 0.003). Considering the upper end (3.3 cm H2O) of the 95% confidence interval and the size of one scale unit (2 cm H2O) of a manometer, the difference in cuff pressure was up to 4 cm H2O in practice.
Conclusions
Even though the air leakage sound disappears on auscultation, unlike the previous recommendation, the airway sealing would be completed only by increasing the cuff pressure by approximately 4 cm H2O.
Figure
-
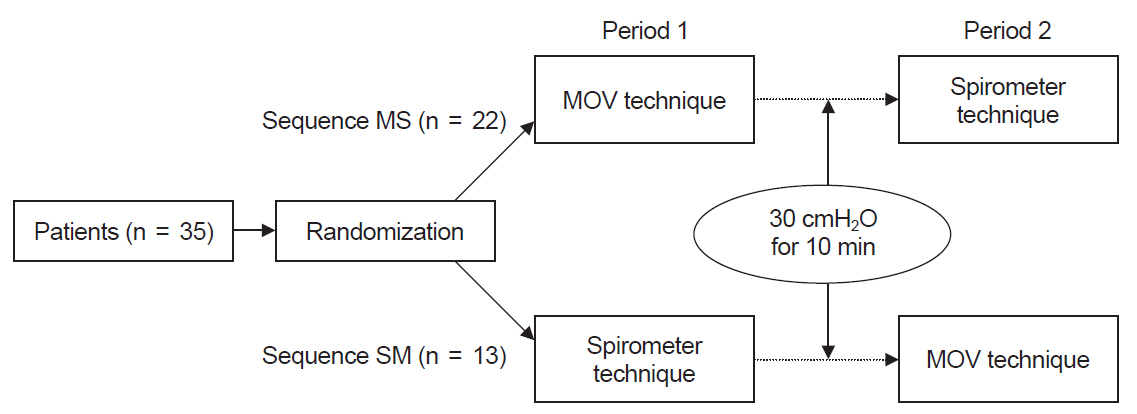
Fig. 1. Study protocol. Patients in Sequence MS received the minimal occlusive volume technique during the first period and the spirometer technique during the second period. Patients in Sequence SM were treated in the reverse order. MOV: minimal occlusive volume.
Reference
-
1. Vyas D, Inweregbu K, Pittard A. Measurement of tracheal tube cuff pressure in critical care. Anaesthesia. 2002; 57:275–7.2. Mahul P, Auboyer C, Jospe R, Ros A, Guerin C, el Khouri Z, et al. Prevention of nosocomial pneumonia in intubated patients: respective role of mechanical subglottic secretions drainage and stress ulcer prophylaxis. Intensive Care Med. 1992; 18:20–5.3. Mandøe H, Nikolajsen L, Lintrup U, Jepsen D, Mølgaard J. Sore throat after endotracheal intubation. Anesth Analg. 1992; 74:897–900.4. Curiel García JA, Guerrero-Romero F, Rodríguez-Morán M. [Cuff pressure in endotracheal intubation: should it be routinely measured?]. Gac Med Mex. 2001; 137:179–82. Spanish.5. Hähnel J, Treiber H, Konrad F, Eifert B, Hahn R, Maier B, et al. [A comparison of different endotracheal tubes. Tracheal cuff seal, peak centering and the incidence of postoperative sore throat]. Anaesthesist. 1993; 42:232–7. German.6. Liu J, Zhang X, Gong W, Li S, Wang F, Fu S, et al. Correlations between controlled endotracheal tube cuff pressure and postprocedural complications: a multicenter study. Anesth Analg. 2010; 111:1133–7.7. Jensen PJ, Hommelgaard P, Søndergaard P, Eriksen S. Sore throat after operation: influence of tracheal intubation, intracuff pressure and type of cuff. Br J Anaesth. 1982; 54:453–7.8. Fernandez R, Blanch L, Mancebo J, Bonsoms N, Artigas A. Endotracheal tube cuff pressure assessment: pitfalls of finger estimation and need for objective measurement. Crit Care Med. 1990; 18:1423–6.9. Braz JR, Navarro LH, Takata IH, Nascimento Júnior P. Endotracheal tube cuff pressure: need for precise measurement. Sao Paulo Med J. 1999; 117:243–7.10. Bolzan DW, Gomes WJ, Faresin SM, de Camargo Carvalho AC, De Paola AA, Guizilini S. Volume-time curve: an alternative for endotracheal tube cuff management. Respir Care. 2012; 57:2039–44.11. Bolzan DW, Gomes WJ, Peixoto TC, Faresin SM, Carvalho AC, De Paola AA, et al. Clinical use of the volume-time curve for endotracheal tube cuff management. Respir Care. 2014; 59:1628–35.12. Almarakbi WA, Kaki AM. Tracheal tube cuff inflation guided by pressure volume loop closure associated with lower postoperative cuff-related complications: prospective, randomized clinical trial. Saudi J Anaesth. 2014; 8:328–34.13. Lizy C, Swinnen W, Labeau S, Poelaert J, Vogelaers D, Vandewoude K, et al. Cuff pressure of endotracheal tubes after changes in body position in critically ill patients treated with mechanical ventilation. Am J Crit Care. 2014; 23:e1–8.14. Al-Metwalli RR, Al-Ghamdi AA, Mowafi HA, Sadek S, Abdulshafi M, Mousa WF. Is sealing cuff pressure, easy, reliable and safe technique for endotracheal tube cuff inflation?: a comparative study. Saudi J Anaesth. 2011; 5:185–9.15. Senn S. Cross-over trials in clinical research. 2nd ed. West Sussex: John Wiley & Sons;2002. p. 35–88.16. American Thoracic Society, Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005; 171:388–416.17. Lorente L, Blot S, Rello J. Evidence on measures for the prevention of ventilator-associated pneumonia. Eur Respir J. 2007; 30:1193–207.18. Hoffman RJ, Parwani V, Hahn IH. Experienced emergency medicine physicians cannot safely inflate or estimate endotracheal tube cuff pressure using standard techniques. Am J Emerg Med. 2006; 24:139–43.19. Parwani V, Hoffman RJ, Russell A, Bharel C, Preblick C, Hahn IH. Practicing paramedics cannot generate or estimate safe endotracheal tube cuff pressure using standard techniques. Prehosp Emerg Care. 2007; 11:307–11.20. Stewart SL, Secrest JA, Norwood BR, Zachary R. A comparison of endotracheal tube cuff pressures using estimation techniques and direct intracuff measurement. AANA J. 2003; 71:443–7.21. Sole ML, Aragon D, Bennett M, Johnson RL. Continuous measurement of endotracheal tube cuff pressure: how difficult can it be? AACN Adv Crit Care. 2008; 19:235–43.22. Blanch PB. Laboratory evaluation of 4 brands of endotracheal tube cuff inflator. Respir Care. 2004; 49:166–73.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Comparison of Passive Release Technique and Minimal Occlusive Volume Technique for Endotracheal Tube Cuff Inflation
- The Effects of Tidal Volume on Minimal Occlusion Pressure of Endotracheal Tube Cuff in Patients with Same Peak Inspiratory pressure
- Endotracheal Tube Cuff Volume and Pressure Changes in the Use of Nitrous Oxide
- Application of a Loss of Resistance Syringe for Obtaining the Adequate Cuff Pressures of Endotracheal Intubated Patients in an Emergency Department
- Repeated endotracheal tube cuff tears during nasotracheal intubation due to nasal cavity orthodontic micro-implant - A case report -
