Stereotactic Cardiac Radiation to Control Ventricular Tachycardia and Fibrillation Storm in a Patient with Apical Hypertrophic Cardiomyopathy at Burnout Stage: Case Report
- Affiliations
-
- 1Department of Cardiology, Dong-A University Hospital, Busan, Korea
- 2Department of Radiation Oncology, Dong-A University Hospital, Busan, Korea
- KMID: 2504259
- DOI: http://doi.org/10.3346/jkms.2020.35.e200
Abstract
- Stereotactic cardiac radiation for ablation (radioablation) of life-threatening ventricular arrhythmia was recently introduced into clinical practice. A 76-year-old male patient with apical hypertrophic cardiomyopathy at burnout stage, who received defibrillator implantation for the secondary prevention of sudden arrhythmic death, was admitted for repeated defibrillator therapy. Radiofrequency catheter ablation was unsuccessful due to the induction of ventricular fibrillation (VF) and hemodynamically unstable sustained monomorphic ventricular tachycardia (VT). However, intracardiac activation mapping for the induced VT revealed the earliest ventricular activation at the apical aneurysm. Radioablation was performed to control VT and VF storm refractory to antiarrhythmic drug therapy. A total of 24 Gray was radiated, divided into three fractions around the apical aneurysm. The onset of electrical modulation was instantaneous and the antiarrhythmic effect was maintained for at least 6 months without significant radiation toxicities. This case suggests that radioablation may be considered as a rescue therapy for VT and VF storm refractory to other treatment modalities.
Keyword
Figure
-
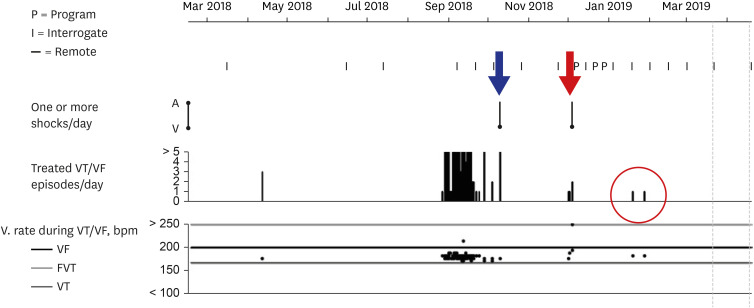
Fig. 1 Report of VT and VF episodes recorded by the patient's ICD.ICD interrogation showed that the number of treated VT episodes/day requiring anti-tachycardia pacing had increased remarkably from September 2018. When ICD shock was delivered in October 2018 (blue arrow), the patient lost consciousness during ICD charging. Because treated VT episodes/day increased again in December 2018, the patient was admitted for ablation. Stereotactic cardiac radiation was performed on 5 December 2018 to control VT and VF storm (red arrow) in which ICD shocks were delivered 7 times for 24 hours. Although sustained VT requiring anti-tachycardia pacing recurred two times at 6 and 8 weeks (red circle) while reducing the doses of antiarrhythmic agents, ICD shock was no longer delivered.VT = ventricular tachycardia, VF = ventricular fibrillation, ICD = implantable cardioverter-defibrillator.
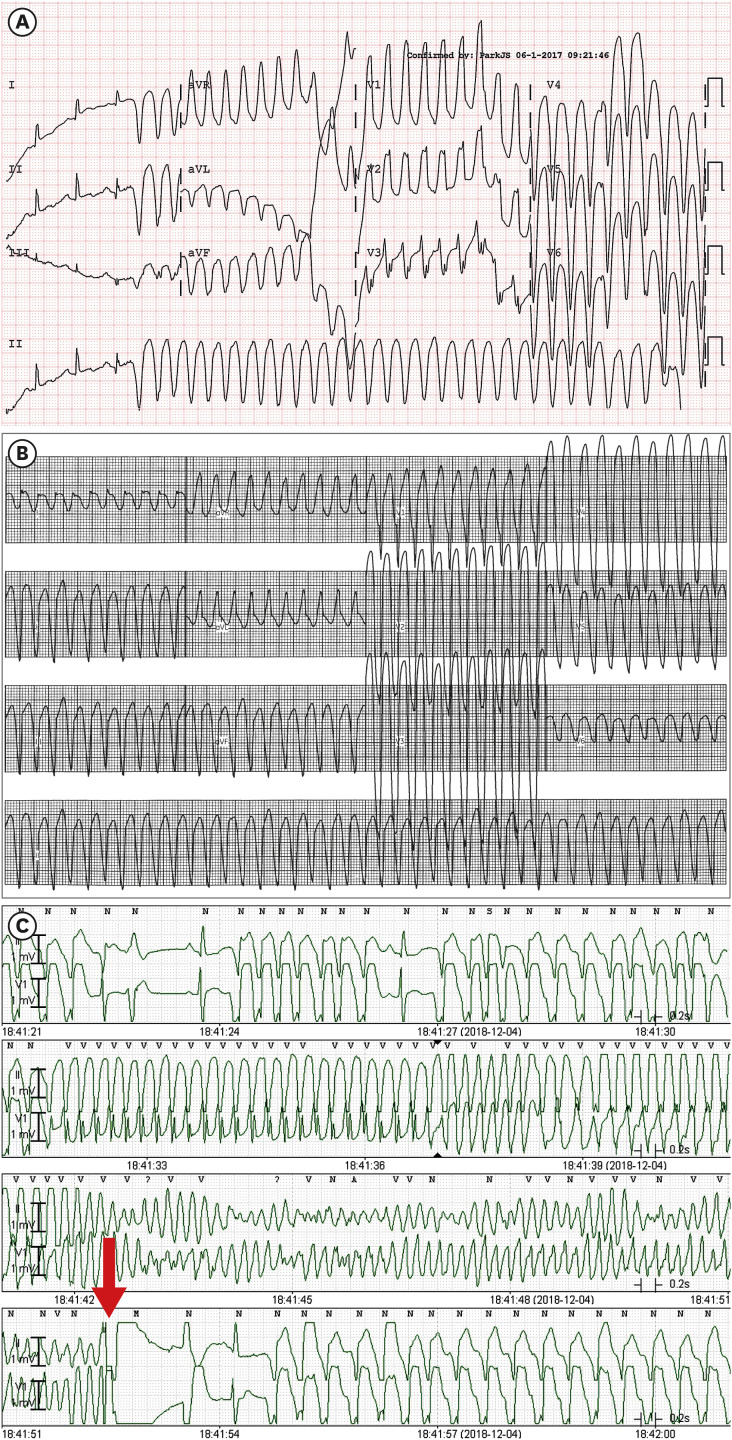
Fig. 2 VT and VF electrocardiographic findings.(A) Sustained monomorphic VT (cycle length, 240 ms; QRS duration, 120 ms) documented 3 years prior to ICD implantation showed a right bundle branch block configuration in the V1 lead, cardiac axis to no man's land, and cardiac transition in the V3 lead, suggesting a left ventricular apicolateral origin. (B) Sustained monomorphic VT (cycle length, 240 ms; QRS duration, 120 ms) induced during the electrophysiologic study showed left bundle branch block configuration in the V1 lead, cardiac axis to no man's land, and negative precordial concordance, which suggested a right ventricular apical or left ventricular apical septal origin. (C) Telemetry recordings showed a recurrence of fast VT and VF, which should be terminated by ICD shock (red arrow).VT = ventricular tachycardia, VF = ventricular fibrillation, ICD = implantable cardioverter-defibrillator.
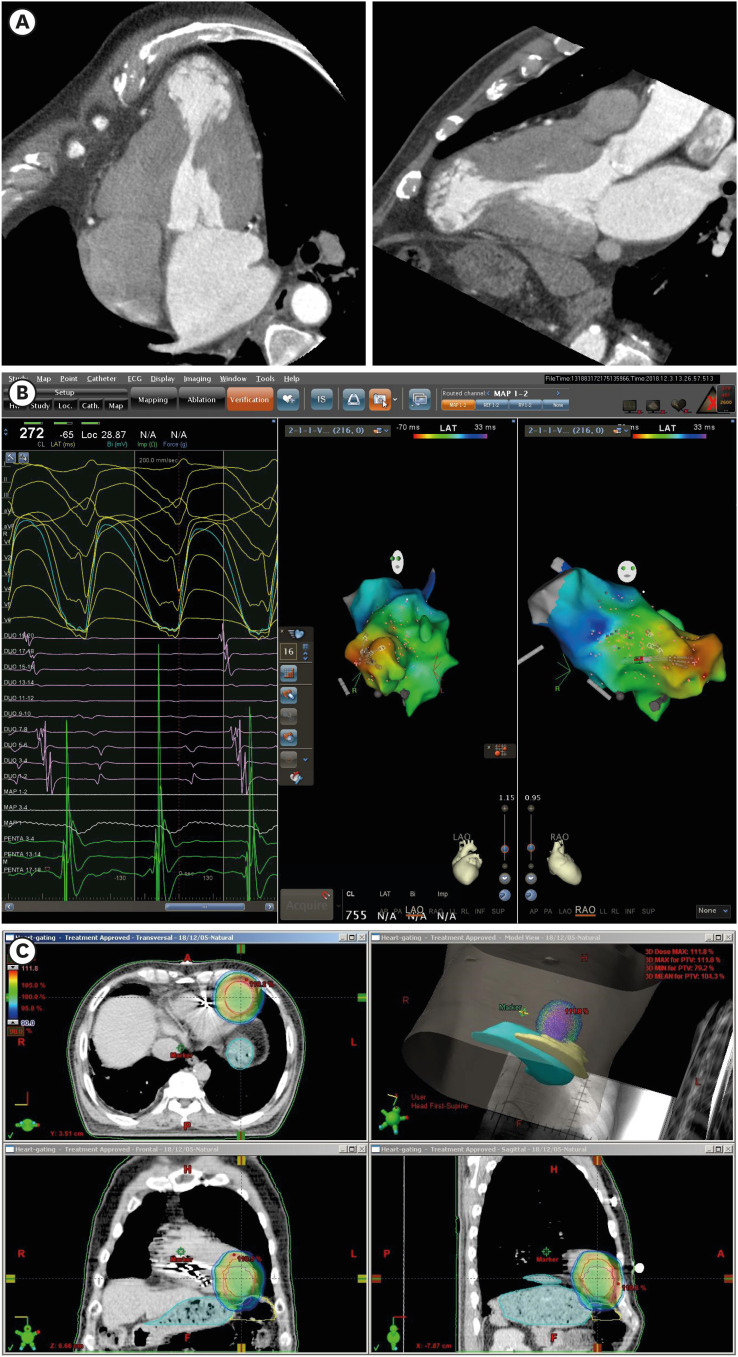
Fig. 3 Electroanatomic targeting of arrhythmogenic substrates for cardiac radioablation.(A) Cardiac multidetector computed tomography images reveal aneurysmal dilation of the cardiac apex compatible with apical hypertrophic cardiomyopathy at burnout stage. (B) Activation mapping of the sustained monomorphic ventricular tachycardia using a multi-electrode mapping catheter and three-dimensional navigation system revealed that ventricular activation (red color) began in the septal side of the LV apical aneurysm and propagated to the LV base (blue color). (C) The gross tumor volume for stereotactic cardiac radiation was defined as the LV apical aneurysm and surrounding myocardium with 1 cm extension from the aneurysmal border. The proximal end of the defibrillator shock coil was used as a radiologic marker for the patient setup.LV = left ventricle.
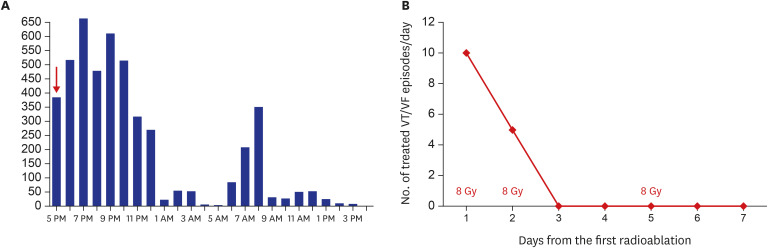
Fig. 4 Response to cardiac radioablation.(A) The first stereotactic cardiac radiation was performed at 5 pm (red arrow). The burden of couplets of the ventricular premature beat recorded by 24-hour ambulatory electrocardiographic monitoring decreased remarkably over the initial 24 hours. (B) A total of 24 Gy was delivered to the planned target volume on the first, second, and fifth days. The number of treated VT/VF episodes/day began to decrease immediately after delivery of the first radiation dose. After delivery of 16 Gy, VT/VF episodes requiring anti-tachycardia pacing or shock therapy did not recur.Gy = Gray, VT = ventricular tachycardia, VF = ventricular fibrillation.
Cited by 1 articles
-
Letter to the Editor: Stereotactic Cardiac Radiation to Control Ventricular Tachycardia and Fibrillation Storm in a Patient with Apical Hypertrophic Cardiomyopathy at Burnout Stage: Case Report
Alvin Oliver Payus, Norlaila Mustafa
J Korean Med Sci. 2020;35(43):e381. doi: 10.3346/jkms.2020.35.e381.
Reference
-
1. Loo BW Jr, Soltys SG, Wang L, Lo A, Fahimian BP, Iagaru A, et al. Stereotactic ablative radiotherapy for the treatment of refractory cardiac ventricular arrhythmia. Circ Arrhythm Electrophysiol. 2015; 8(3):748–750. PMID: 26082532.
Article2. Cuculich PS, Schill MR, Kashani R, Mutic S, Lang A, Cooper D, et al. Noninvasive cardiac radiation for ablation of ventricular tachycardia. N Engl J Med. 2017; 377(24):2325–2336. PMID: 29236642.
Article3. Robinson CG, Samson PP, Moore KM, Hugo GD, Knutson N, Mutic S, et al. Phase I/II trial of electrophysiology-guided noninvasive cardiac radioablation for ventricular tachycardia. Circulation. 2019; 139(3):313–321. PMID: 30586734.
Article4. Benedict SH, Yenice KM, Followill D, Galvin JM, Hinson W, Kavanagh B, et al. Stereotactic body radiation therapy: the report of AAPM Task Group 101. Med Phys. 2010; 37(8):4078–4101. PMID: 20879569.
Article5. Sharma A, Wong D, Weidlich G, Fogarty T, Jack A, Sumanaweera T, et al. Noninvasive stereotactic radiosurgery (CyberHeart) for creation of ablation lesions in the atrium. Heart Rhythm. 2010; 7(6):802–810. PMID: 20156591.
Article6. Lehmann HI, Graeff C, Simoniello P, Constantinescu A, Takami M, Lugenbiel P, et al. Feasibility study on cardiac arrhythmia ablation using high-energy heavy ion beams. Sci Rep. 2016; 6(1):38895. PMID: 27996023.
Article7. Refaat MM, Ballout JA, Zakka P, Hotait M, Al Feghali KA, Gheida IA, et al. Swine atrioventricular node ablation using stereotactic radiosurgery: methods and in vivo feasibility investigation for catheter-free ablation of cardiac arrhythmias. J Am Heart Assoc. 2017; 6(11):e007193. PMID: 29079566.
Article8. Zei PC, Wong D, Gardner E, Fogarty T, Maguire P. Safety and efficacy of stereotactic radioablation targeting pulmonary vein tissues in an experimental model. Heart Rhythm. 2018; 15(9):1420–1427. PMID: 29678783.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Letter to the Editor: Stereotactic Cardiac Radiation to Control Ventricular Tachycardia and Fibrillation Storm in a Patient with Apical Hypertrophic Cardiomyopathy at Burnout Stage: Case Report
- Mid-Ventricular Hypertrophic Obstructive Cardiomyopathy Complicated by an Apical Aneurysm, Presenting as Ventricular Tachycardia
- Mid-Septal Hypertrophy and Apical Ballooning; Potential Mechanism of Ventricular Tachycardia Storm in Patients with Hypertrophic Cardiomyopathy
- 4 Cases of Midventricular Obstructive Hypertrophic Obstructive Cardiomyopathy
- A Case of Regressed Apical Hypertrophic Cardiomyopathy
