Validation of a Novel Endoscopic Retrograde Cholangiopancreatography Cannulation Simulator
- Jirapinyo P
 1,2
1,2 - Thompson AC2
- Aihara H1,2
- Ryou M1,2
- Thompson CC1,2
- Affiliations
-
- 1Division of Gastroenterology, Hepatology and Endoscopy, Brigham and Women’s Hospital, Boston, MA, USA
- 2Harvard Medical School, Boston, MA, USA
- KMID: 2502770
- DOI: http://doi.org/10.5946/ce.2019.105
Abstract
- Background/Aims
Endoscopic retrograde cholangiopancreatography (ERCP) requires a unique skill set. Currently, there is no objective methodology to assess and train a professional to perform ERCP. This study aimed to develop and validate a novel ERCP simulator.
Methods
The simulator consists of papillae presenting different anatomy and positioned in varied locations. Deep cannulation of the pancreatic duct, followed by the bile duct, was performed. The time allotted was 5 minutes. The content validity indexes (CVIs) for realism, relevance, and representativeness were calculated. Correlation between ERCP experience and simulator score was determined.
Results
Twenty-three participants completed the simulation. The CVIs for realism were orientation of duodenoscope to papilla (1.00), angulation of papillotome to achieve cannulation (0.71), and haptic feedback during cannulation (0.80). The CVIs for relevance were use of elevator (1.00), wheels to achieve en face orientation (1.00), and papillotome for selective cannulation (1.00). Regarding CVI for representativeness, the results were as follows: basic cannulation (0.83), papilla locations (0.83), and papilla anatomies (0.80). The novice, intermediate, and experienced groups scored 6.7±8.7, 30.0±16.3, and 74.4±43.9, respectively (p<0.0001). There was a strong correlation between the ERCP experience level and the individual’s simulator score (Pearson value of 0.77, R2 of 0.60).
Conclusions
This simulator appears to be realistic, relevant, and representative of ERCP cannulation techniques. Additionally, it is effective at objectively assessing basic ERCP skills by differentiating scores based on clinical experience.
Keyword
Figure
-
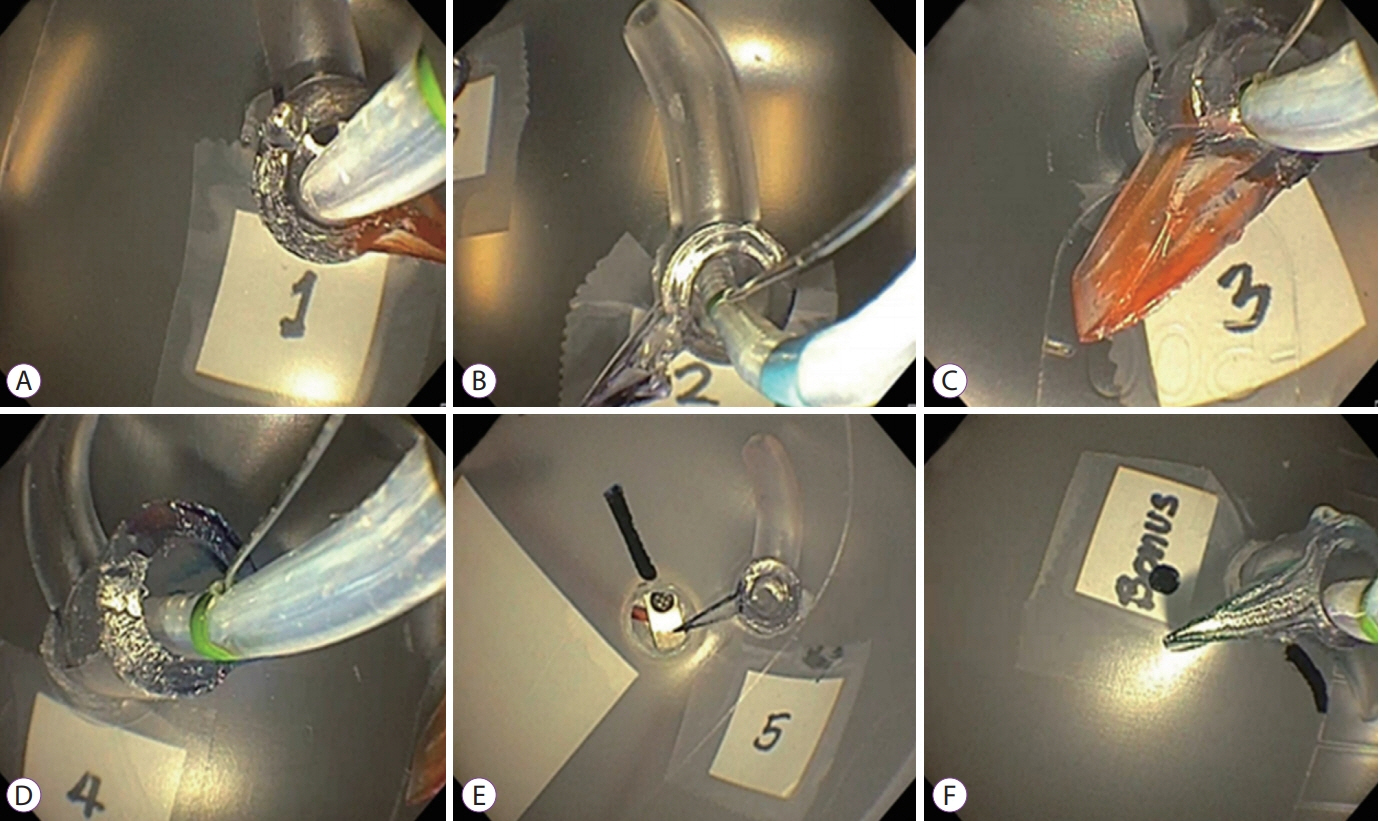
Fig. 1. Endoscopic retrograde cholangiopancreatography Simulator. (A) Papilla in a proximal second portion of the duodenum (D2) position. (B) Papilla in a distal D2 position. (C) Papilla in a standard D2 position. (D) Papilla in a standard D2 position with a long common channel and slightly off axis. (E) Papilla in a supine position. (F) Papilla in a Billroth II and Roux-en-Y gastric bypass anatomy. For papillae 1–5, a standard sphincterotome is used for cannulation. Only operators who successfully cannulate papillae 1–5 within 5 minutes are allowed to advance to papilla 6; a standard sphincterotome (shown), a cannulation catheter, or a flexible tip cannula may be used to achieve cannulation of this bonus papilla.

Fig. 2. Schematic drawing of simulated papilla. Each papilla differs by the length of the common channel (X), the angle between the bile duct and the pancreatic duct (Y), and the axis of the bile duct (Z)

Fig. 3. Complete endoscopic retrograde cholangiopancreatography simulator and room setup.

Fig. 4. Correlation between endoscopic retrograde cholangiopancreatography (ERCP) experience levels and simulator scores. (A) Differentiation of ERCP simulator scores among experience levels. (B) Correlation between the number of ERCPs previously performed and simulator scores. Data presented as mean±standard error.
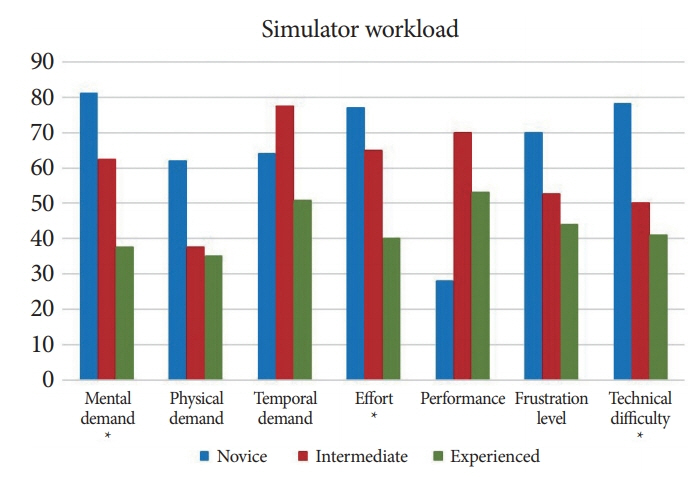
Fig. 5. Endoscopic retrograde cholangiopancreatography simulator workload as assessed by the NASA Task Load Index. *Represents statistically significant difference among the 3 groups (novice, intermediate and experienced)
Reference
-
1. Andriulli A, Loperfido S, Napolitano G, et al. Incidence rates of post-ERCP complications: a systematic survey of prospective studies. Am J Gastroenterol. 2007; 102:1781–1788.
Article2. Freeman ML, Nelson DB, Sherman S, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996; 335:909–918.
Article3. Masci E, Toti G, Mariani A, et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol. 2001; 96:417–423.
Article4. Chutkan RK, Ahmad AS, Cohen J, et al. ERCP core curriculum. Gastrointest Endosc. 2006; 63:361–376.
Article5. Desilets DJ, Banerjee S, Barth BA, et al. Endoscopic simulators. Gastrointest Endosc. 2011; 73:861–867.
Article6. Matthes K, Cohen J. The Neo-Papilla: a new modification of porcine ex vivo simulators for ERCP training (with videos). Gastrointest Endosc. 2006; 64:570–576.
Article7. Neumann M, Mayer G, Ell C, et al. The Erlangen Endo-Trainer: lifelike simulation for diagnostic and interventional endoscopic retrograde cholangiography. Endoscopy. 2000; 32:906–910.
Article8. Sedlack R, Petersen B, Binmoeller K, Kolars J. A direct comparison of ERCP teaching models. Gastrointest Endosc. 2003; 57:886–890.
Article9. Bittner JG 4th, Mellinger JD, Imam T, Schade RR, Macfadyen BV Jr. Face and construct validity of a computer-based virtual reality simulator for ERCP. Gastrointest Endosc. 2010; 71:357–364.10. Thompson CC, Jirapinyo P, Kumar N, et al. Development and initial validation of an endoscopic part-task training box. Endoscopy. 2014; 46:735–744.
Article11. Jirapinyo P, Kumar N, Thompson CC. Validation of an endoscopic part-task training box as a skill assessment tool. Gastrointest Endosc. 2015; 81:967–973.
Article12. Jirapinyo P, Abidi WM, Aihara H, et al. Preclinical endoscopic training using a part-task simulator: learning curve assessment and determination of threshold score for advancement to clinical endoscopy. Surg Endosc. 2017; 31:4010–4015.
Article13. American Educational Research Association; American Psychological Association; National Council on Measurement in Education; Joint Committee on Standards for Educational and Psychological Testing (U.S.). Standards for educational and psychological testing. Washington, D.C.: American Educational Research Association;1999.14. Downing SM. Validity: on meaningful interpretation of assessment data. Med Educ. 2003; 37:830–837.15. American Association for the Study of Liver Diseases; American College of Gastroenterology; American Gastroenterological Association (AGA) Institute; American Society for Gastrointestinal Endoscopy. The gastroenterology core curriculum, Third edition. Gastroenterology. 2007; 132:2012–2018.16. Hart SG. NASA Task Load Index (TLX). vol. 1.0. paper and pencil package. Moffett Field (CA): NASA Ames Research Center;1986. p. 26.17. Hart SG, Staveland LE. NASA Task Load Index (TLX). vol. 1.0. paper and pencil package. Moffett Field (CA): NASA Ames Research Center;1986. p. 136–183.18. Adler DG, Lieb JG 2nd, Cohen J, et al. Quality indicators for ERCP. Gastrointest Endosc. 2015; 81:54–66.
Article19. Wani S, Keswani RN, Petersen B, et al. Training in EUS and ERCP: standardizing methods to assess competence. Gastrointest Endosc. 2018; 87:1371–1382.
Article20. Leung JW, Yen D. ERCP training - the potential role of simulation practice. J Interv Gastroenterol. 2011; 1:14–18.
Article21. Frimberger E, von Delius S, Rösch T, Karagianni A, Schmid RM, Prinz C. A novel and practicable ERCP training system with simulated fluoroscopy. Endoscopy. 2008; 40:517–520.
Article22. von Delius S, Thies P, Meining A, et al. Validation of the X-Vision ERCP training system and technical challenges during early training of sphincterotomy. Clin Gastroenterol Hepatol. 2009; 7:389–396.
Article23. Boškoski I, Costamagna G. The Boskoski-Costamagna ERCP trainer: from dream to reality. Endoscopy. 2016; 48:593.24. van der Wiel SE, Koch AD, Bruno MJ. Face and construct validity of a novel mechanical ERCP simulator. Endosc Int Open. 2018; 6:E758–E765.
Article25. Downing SM, Haladyna TM. Validity threats: overcoming interference with proposed interpretations of assessment data. Med Educ. 2004; 38:327–333.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prevention of Post-endoscopic Retrograde Cholangiopancreatography Pancreatitis: An Endoscopic Perspective
- Optimal Use of Wire-Assisted Techniques and Precut Sphincterotomy
- Prevention of Postendoscopic Retrograde Cholangiopancreatography Pancreatitis: The Endoscopic Technique
- Successful Selective Biliary Cannulation Using Biopsy Forceps during Endoscopic Retrograde Cholangiopancreatography: A Case Report
- The Usefulness of Cap-assisted Endoscopic Retrograde Cholangiopancreatography for Cannulation Complicated by a Periampullary Diverticulum
