One Stage Microsurgical Reconstruction with Chimeric Flap for Salvaging a Complex Hand Injuries
- Affiliations
-
- 1Reconstructive Sciences Unit, Hospital Universiti Sains Malaysia, Kubang Kerian, Kelantan, Malaysia
- 2Orthopedic Oncology and Reconstructive Unit, Department of Orthopaedics, Hospital Universiti Sains Malaysia, Kubang Kerian, Kelantan, Malaysia
- 3Plastic and Reconstructive Unit, MSU Medical Center, Shah Alam, Selangor, Malaysia
- KMID: 2502714
- DOI: http://doi.org/10.12790/ahm.20.0007
Abstract
- Hand injuries, involving extensor tendon with carpal bone loss are catastrophic events. Reconstructive surgeons typically face difficulties in minimizing the number of operations, recovery period and restoring its functions with an acceptable aesthetic outcome. However, chimeric flap, which consists of multiple composite flaps from one of the sources of main vascular system is a promising option for reconstruction. This paper presents a case of near-amputated degloving injury over the extensor tendon with carpal bone loss on left hand due to road traffic accidents. The patient had a hand reconstruction with chimeric flap consisted of free fasciocutaneous anterolateral thigh flap and vascularized osteomyocutaneous iliac bone graft with tensor fascia lata from the lateral circumflex femoral vascular system. As a result, the hand functioned well and appeared aesthetically acceptable. Thus, this surgery is an effective option in recovering and reconstructing a complex and traumatic hand injury that involved multiple composite tissue defects.
Keyword
Figure
-
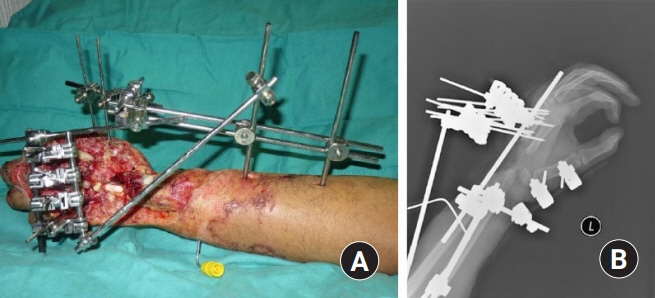
Fig. 1. (A) Left forearm wound and (B) X-ray of left forearm, lateral view.
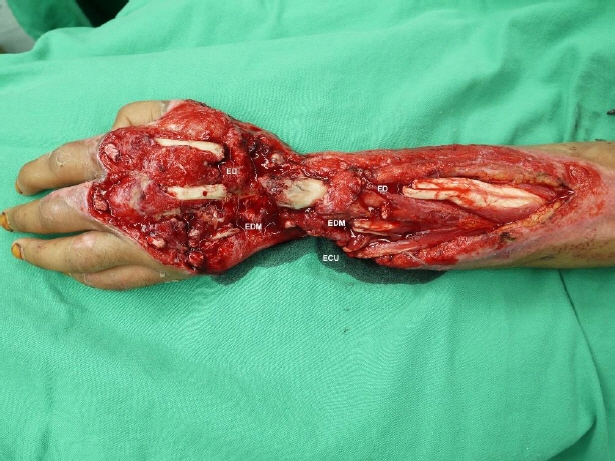
Fig. 2. Defects wound after debridement. ED, extensor digitorum; EDM, extensor digiti minimi; ECU, extensor carpi ulnaris.
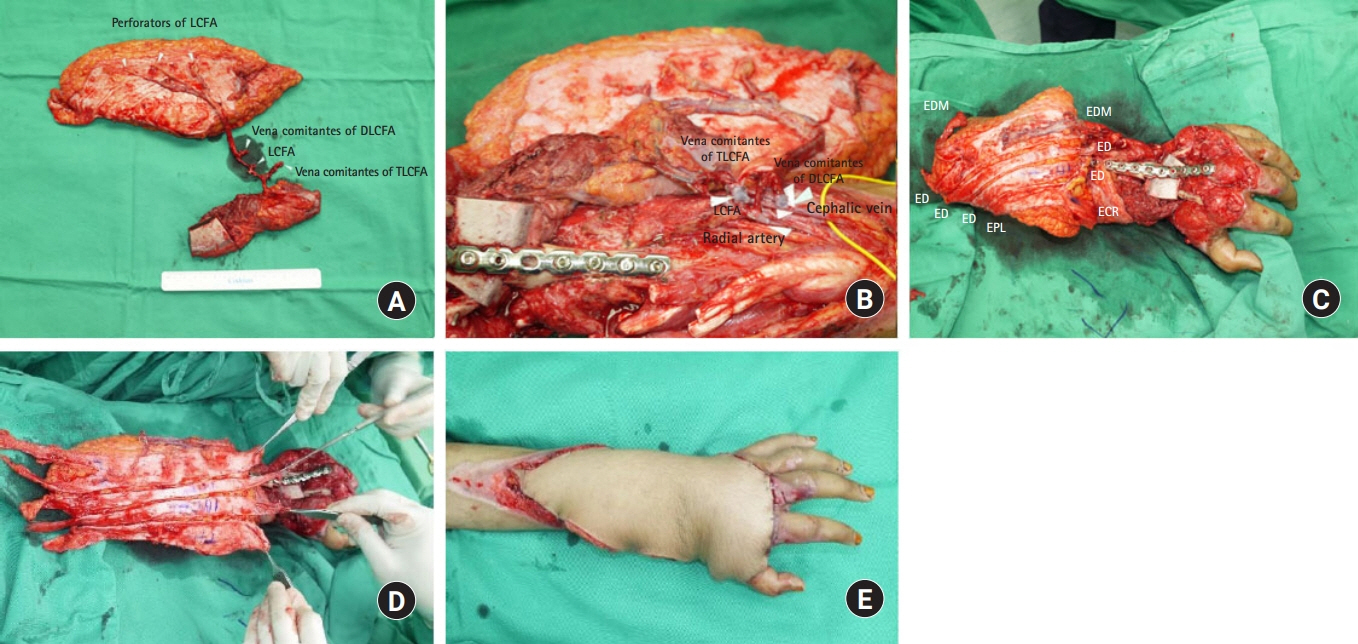
Fig. 3. (A) Chimeric flap of free fasciocutaneous anterolateral thigh flap with fascia lata and vascularized osteomyocutaneous iliac bone graft. (B) Vascular anastomoses between recipient and donor vessels. (C) Vascularized iliac bone graft was inserted to cover the carpal bone defect and K-wire was inserted from the metacarpal bone through iliac bone graft. Locking plate was applied across the metacarpal bone. (D) Fascia lata slit into small strips and laid down on top of bone as vascularised tendon grafts for the extensor tendon defects. (E) Immediate result after flap inset. LCFA, lateral circumflex femoral artery; TLCFA, transverse branch of LCFA; DLCFA, descending branch of LCFA.

Fig. 4. Flap debulking and tenolysis surgery.

Fig. 5. (A) Dorsum part of the left forearm in full extensor. (B) Stiffness of ring and little fingers of left hand. (C) X-ray of left forearm after 1 year, anteroposterior view.
Reference
-
1. Koul AR, Patil RK, Philip V. Complex extensor tendon injuries: early active motion following single-stage reconstruction. J Hand Surg Eur Vol. 2008; 33:753–9.2. Baker SR. Reconstruction of mandibular defects with the revascularized free tensor fascia lata osteomyocutaneous flap. Arch Otolaryngol. 1981; 107:414–8.
Article3. Pan ZH, Jiang PP, Xue S, Li H, Wang JL. Restoration of basic hand function following devastating hand injuries using a microsurgically fabricated chimeric iliac osteocutaneous flap. J Plast Reconstr Aesthet Surg. 2017; 70:723–8.
Article4. Pan ZH, Jiang PP, Zhao YX, Wang JL. Treatment of complex metacarpal defects with free chimeric iliac osteocutaneous flaps. J Plast Surg Hand Surg. 2017; 51:143–8.
Article5. Huang WC, Chen HC, Wei FC, Cheng MH, Schnur DP. Chimeric flap in clinical use. Clin Plast Surg. 2003; 30:457–67.
Article6. Meky M. Versatility of anterolateral thigh flap in dorsal hand reconstruction. AAMJ. 2015; 13(Suppl 2):108–13.7. Iyer S, Chatni S, Kuriakose MA. Free tensor fascia lata-iliac crest osteomusculocutaneous flap for reconstruction of combined maxillectomy and orbital floor defect. Ann Plast Surg. 2012; 68:52–7.
Article8. Kremer T, Bickert B, Germann G, Heitmann C, Sauerbier M. Outcome assessment after reconstruction of complex defects of the forearm and hand with osteocutaneous free flaps. Plast Reconstr Surg. 2006; 118:443–56.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hand Reconstruction Using Medialis Pedis and Medial Plantar Chimeric Free Flap
- Immediate Microsurgical Reconstruction of Fingertip Injuries
- Microsurgical reconstruction for traumatic hand defects in pediatric patients
- Reconstruction of a Mangled Hand with a Thoracodorsal Artery Perforator Free Flap: A Report of Two Cases
- Microsurgical Reconstruction of Lower Limb Using Thoracodorsal Artery Perforator Chimeric Free Flap after Popliteal Artery Revascularization: A Case Report
