J Dent Anesth Pain Med.
2020 Feb;20(1):45-47. 10.17245/jdapm.2020.20.1.45.
Endotracheal tube damage during surgically assisted rapid palatal expansion surgery; a case report
- Affiliations
-
- 1University Hospital Southampton NHS Foundation Trust, University of Southampton, Southampton, United Kingdom. j.e.g.badger@soton.ac.uk
- KMID: 2471173
- DOI: http://doi.org/10.17245/jdapm.2020.20.1.45
Abstract
- Endotracheal tube damage is a well-known complication of maxillary surgery. We report a case of failure to ventilate due to superficial damage to the tubing between the cuff and pilot balloon in the nasal portion of a north facing Ring, Adair and Elwyn pre-formed endotracheal tube during Surgically Assisted Rapid Palatal Expansion surgery. The endotracheal tube was replaced uneventfully and surgery completed successfully. On reflection, we feel that that the vulnerable position of the cuff-pilot tubing significantly contributed to this critical incident and suggest that increased recognition of this is vital for the prevention of such cases in the future.
Keyword
Figure
-

Fig. 1 A photograph of the damaged endotracheal tube
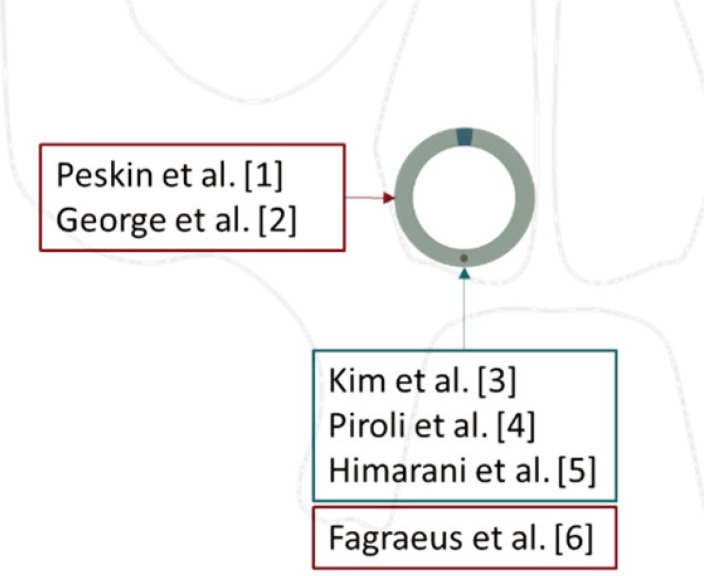
Fig. 2 Location and extent of endotracheal tube damage. The grey outline represents a coronal section of the face. The circle is a transverse section of a pre-formed endotracheal tube in situ with the cuff to pilot balloon tubing within the lower border (black circle). The blue box represents studies where superficial damage to the endotracheal tube has been clinically significant due to cuff deflation. The red boxes represent the location of clinically significant damage as a result of > 50% transection.
Reference
-
1. Peskin RM, Sachs SA. Intraoperative management of a partially severed endotracheal tube during orthognathic surgery. Anesth Prog. 1986; 33:247–251. PMID: 3465262.2. George P, Fiadjoe JE, Simpao AF. An unusual lacerated tracheal tube during Le Fort surgery: literature review and case report. Case Rep Anesthesiol. 2016; 2016:6298687. PMID: 27895942.
Article3. Kim EJ, Yoon JY, Woo MN, Kim CH, Yoon JU, Jeon DN. Damage to the pilot balloon of the nasotracheal tube during orthognathic double-jaw surgery: A case report. J Dent Anesth Pain Med. 2015; 15:101–103. PMID: 28879266.
Article4. Piroli A, Cutilli T, Lupi E, Marinangeli F, Varrassi G, Paladini A. Different solutions for damaged nasotracheal tube during maxillofacial surgery: a case series. Adv Ther. 2019; 36:1812–1816. PMID: 31065994.
Article5. Himarani J, Nancy SM, Krishna Kumar Raja VB, Shanmuga Sundaram S. Management of an intraoperatively damaged endotracheal tube in a case of difficult airway using fibre-optic bronchoscope with minimal apnoea period. Indian J Anaesth. 2017; 61:347–349. PMID: 28515525.
Article6. Fagraeus L, Angelillo JC, Dolan EA. A serious anesthetic hazard during orthognathic surgery. Anesth Analg. 1980; 59:150–153. PMID: 6989286.
Article7. Adke M, Mendonca C. Concealed airway complication during LeFort I osteotomy. Anaesthesia. 2003; 58:294–295.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgically assisted rapid palatal expansion with tent screws and a custom-made palatal expander: a case report
- A posteroanterior cephalometric study on the change of maxilla by rapid palatal expansion
- Crowding with no posterior crossbite treatment byrapid palatal expansion
- Surgically assisted rapid maxillary expansion and orthognathic treatments: report of 2 cases
- Surgically Assisted Rapid Maxillary Expansion: Report Of 5 Cases
