Anatomic Evaluation of the Interportal Capsulotomy Made with the Modified Anterior Portal versus Standard Anterior Portal: Comparable Utility with Decreased Capsule Morbidity
- Affiliations
-
- 1USC Epstein Family Center for Sports Medicine at Keck Medicine of USC, Los Angeles, CA, USA. weberae@usc.edu
- 2Division of Sports Medicine, Department of Orthopedic Surgery, Henry Ford Health System, Detroit, MI, USA.
- 3Department of Orthopedic Surgery, University of California, Los Angeles, Los Angeles, CA, USA.
- 4Department of Orthopaedics and Sports Medicine, Houston Methodist Hospital, Houston, TX, USA.
- 5Midwest Orthopaedics at Rush, Chicago, IL, USA.
- KMID: 2471130
- DOI: http://doi.org/10.5371/hp.2020.32.1.42
Abstract
- PURPOSE
To identify potential differences in interportal capsulotomy size and cross-sectional area (CSA) using the anterolateral portal (ALP) and either the: (i) standard anterior portal (SAP) or (ii) modified anterior portal (MAP).
MATERIALS AND METHODS
Ten cadaveric hemi pelvis specimens were included. A standard arthroscopic ALP was created. Hips were randomized to SAP (n=5) or MAP (n=5) groups. The spinal needle was placed at the center of the anterior triangle or directly adjacent to the ALP in the SAP and MAP groups, respectively. A capsulotomy was created by inserting the knife through the SAP or MAP. The length and width of each capsulotomy was measured using digital calipers under direct visualization. The CSA and length of the capsulotomy as a percentage of total iliofemoral ligament (IFL) side-to-side width were calculated.
RESULTS
There were no differences in mean cadaveric age, weight or IFL dimensions between the groups. Capsulotomy CSA was significantly larger in the SAP group compared with the MAP group (SAP 2.16±0.64 cm2 vs. MAP 0.65±0.17 cm2, P=0.008). Capsulotomy length as a percentage of total IFL width was significantly longer in the SAP group compared with the MAP group (SAP 74.2±14.1% vs. MAP 32.4±3.7%, P=0.008).
CONCLUSION
The CSA of the capsulotomy and the percentage of the total IFL width disrupted are significantly smaller when the interportal capsulotomy is performed between the ALP and MAP portals, compared to the one created between the ALP and SAP. Surgeons should be aware of this fact when performing hip arthroscopy.
Keyword
Figure
-
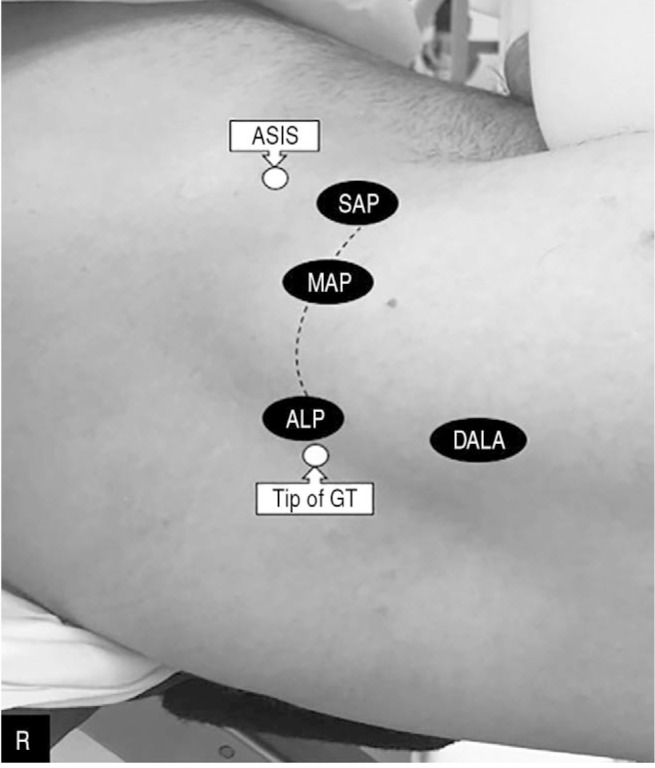
Fig. 1 Demonstration of the superficial landmarks and common arthroscopic portals used to correct femoroacetabular impingement lesions on a right (R) hip: anterolateral portal (ALP), mid-anterior portal (MAP), and standard anterior portal (SAP), distal anterolateral portal (DALA), greater trochanter (GT), anterior superior iliac spine (ASIS). The line demonstrates the connection between ALP-MAP versus ALP-SAP which is performed during the interportal capsulotomy.
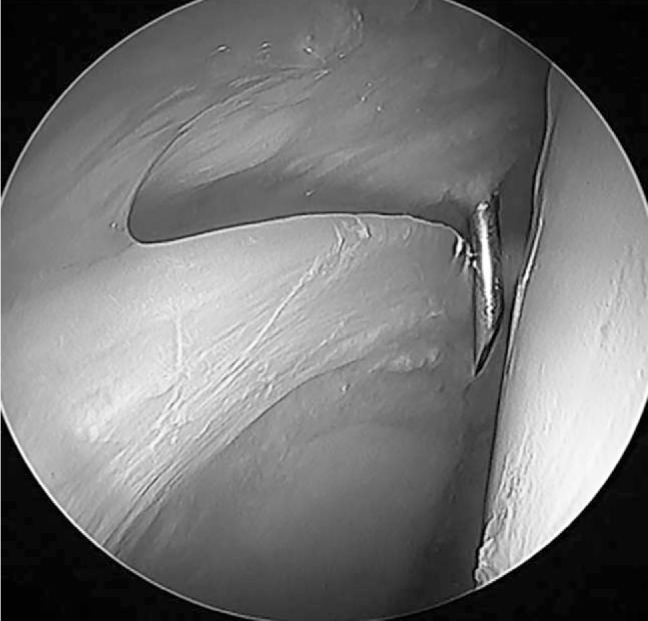
Fig. 2 Arthroscopic image demonstrating placement of the spinal needle at the center of the anterior triangle to create the standard anterior portal interportal capsulotomy.
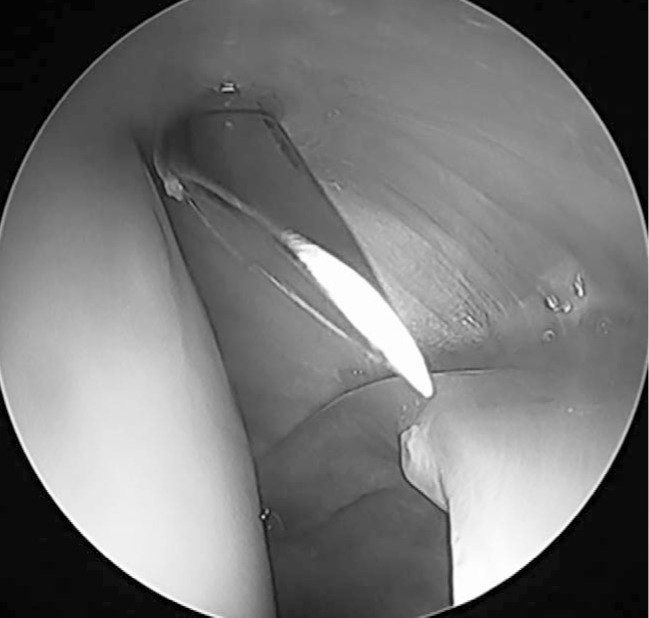
Fig. 3 Arthroscopic image demonstrating placement of the spinal needle into the central compartment to create the modified anterior portal interportal capsulotomy. The spinal needle is inserted such that it can touch the arthroscopic camera cannula.
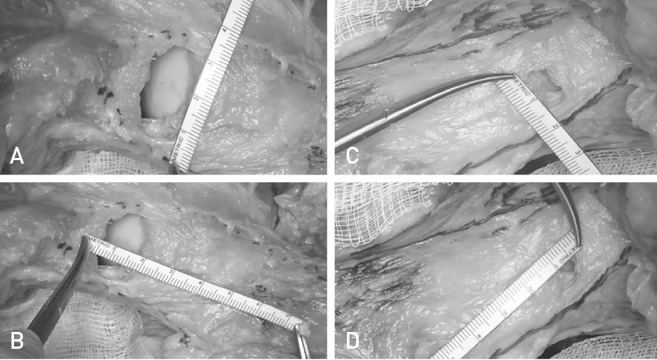
Fig. 4 (A) Measurement of the standard anterior portal (SAP) interportal capsulotomy length. (B) Measurement of the SAP interportal capsulotomy width. (C) Measurement of the modified anterior portal (MAP) interportal capsulotomy length. (D) Measurement of the MAP interportal capsulotomy width.
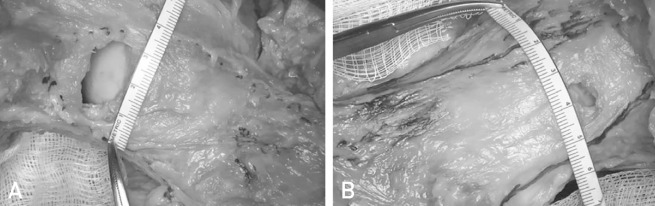
Fig. 5 (A) Measurement of the iliofemoral ligament (IFL) side-to-side width at the level of the capsulotomy allowing for the width of the standard anterior portal interportal capsulotomy to be expressed as a percentage of total IFL. (B) Measurement of the IFL side-to-side width at the level of the capsulotomy allowing for the width of the modified anterior portal interportal capsulotomy to be expressed as a percentage of total IFL.
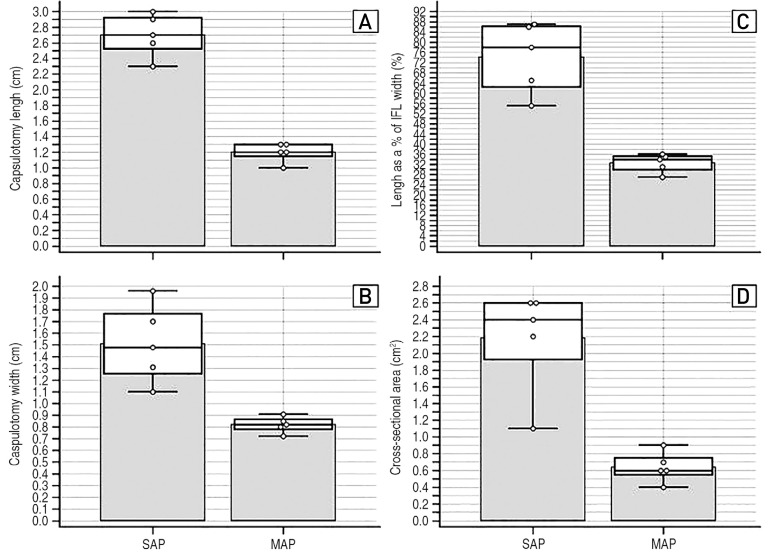
Fig. 6 Plotting distribution of the measurements in the modified anterior portal (MAP) versus standard anterior portal (SAP) groups: (A) Capsulotomy length. (B) Capsulotomy width. (C) Length of capsulotomy as a percentage of iliofemoral ligament (IFL) width. (D) Cross-sectional area of the anterolateral portal (ALP)-SAP and ALP-MAP capsulotomy.
Reference
-
1. Burman MS. Arthroscopy or the direct visualization of joints: an experimental cadaver study. J Bone Joint Surg. 1931; 13:669–695.2. Colvin AC, Harrast J, Harner C. Trends in hip arthroscopy. J Bone Joint Surg Am. 2012; 94:e23. PMID: 22336982.
Article3. de SA D, Cargnelli S, Catapano M, et al. Efficacy of hip arthroscopy for the management of septic arthritis: a systematic review. Arthroscopy. 2015; 31:1358–1370. PMID: 25703285.
Article4. Nwachukwu BU, Rebolledo BJ, McCormick F, Rosas S, Harris JD, Kelly BT. Arthroscopic versus open treatment of femoroacetabular impingement: a systematic review of medium- to long-term outcomes. Am J Sports Med. 2016; 44:1062–1068. PMID: 26059179.5. Minkara AA, Westermann RW, Rosneck J, Lynch TS. Systematic review and meta-analysis of outcomes after hip arthroscopy in femoroacetabular impingement. Am J Sports Med. 2019; 47:488–500. PMID: 29373805.
Article6. Menge TJ, Briggs KK, Dornan GJ, McNamara SC, Philippon MJ. Survivorship and outcomes 10 years following hip arthroscopy for femoroacetabular impingement: labral debridement compared with labral repair. J Bone Joint Surg Am. 2017; 99:997–1004. PMID: 28632588.7. Weber AE, Harris JD, Nho SJ. Complications in hip arthroscopy: a systematic review and strategies for prevention. Sports Med Arthrosc Rev. 2015; 23:187–193. PMID: 26524553.8. Cvetanovich GL, Chalmers PN, Levy DM, et al. Hip arthroscopy surgical volume trends and 30-day postoperative complications. Arthroscopy. 2016; 32:1286–1292. PMID: 27067059.
Article9. Cvetanovich GL, Harris JD, Erickson BJ, Bach BR Jr, Bush-Joseph CA, Nho SJ. Revision hip arthroscopy: a systematic review of diagnoses, operative findings, and outcomes. Arthroscopy. 2015; 31:1382–1390. PMID: 25703289.
Article10. McCormick F, Slikker W 3rd, Harris JD, et al. Evidence of capsular defect following hip arthroscopy. Knee Surg Sports Traumatol Arthrosc. 2014; 22:902–905. PMID: 23851921.
Article11. Benali Y, Katthagen BD. Hip subluxation as a complication of arthroscopic debridement. Arthroscopy. 2009; 25:405–407. PMID: 19341928.
Article12. Duplantier NL, McCulloch PC, Nho SJ, Mather RC 3rd, Lewis BD, Harris JD. Hip dislocation or subluxation after hip arthroscopy: a systematic review. Arthroscopy. 2016; 32:1428–1434. PMID: 27090723.
Article13. Wylie JD, Beckmann JT, Maak TG, Aoki SK. Arthroscopic capsular repair for symptomatic hip instability after previous hip arthroscopic surgery. Am J Sports Med. 2016; 44:39–45. PMID: 26419897.
Article14. Yeung M, Memon M, Simunovic N, Belzile E, Philippon MJ, Ayeni OR. Gross instability after hip arthroscopy: an analysis of case reports evaluating surgical and patient factors. Arthroscopy. 2016; 32:1196–1204.e1. PMID: 27013107.
Article15. Bedi A, Galano G, Walsh C, Kelly BT. Capsular management during hip arthroscopy: from femoroacetabular impingement to instability. Arthroscopy. 2011; 27:1720–1731. PMID: 22047925.
Article16. Weber AE, Kuhns BD, Cvetanovich GL, et al. Does the hip capsule remain closed after hip arthroscopy with routine capsular closure for femoroacetabular impingement? A magnetic resonance imaging analysis in symptomatic postoperative patients. Arthroscopy. 2017; 33:108–115. PMID: 27720303.
Article17. Abrams GD, Hart MA, Takami K, et al. Biomechanical evaluation of capsulotomy, capsulectomy, and capsular repair on hip rotation. Arthroscopy. 2015; 31:1511–1517. PMID: 25882176.
Article18. Khair MM, Grzybowski JS, Kuhns BD, Wuerz TH, Shewman E, Nho SJ. The effect of capsulotomy and capsular repair on hip distraction: a cadaveric investigation. Arthroscopy. 2017; 33:559–565. PMID: 28012635.
Article19. Myers CA, Register BC, Lertwanich P, et al. Role of the acetabular labrum and the iliofemoral ligament in hip stability: an in vitro biplane fluoroscopy study. Am J Sports Med. 2011; 39 Suppl:85S–91S. PMID: 21709037.20. Wuerz TH, Song SH, Grzybowski JS, et al. Capsulotomy size affects hip joint kinematic stability. Arthroscopy. 2016; 32:1571–1580. PMID: 27212048.
Article21. Chahla J, Mikula JD, Schon JM, et al. Hip capsular closure: a biomechanical analysis of failure torque. Am J Sports Med. 2017; 45:434–439. PMID: 27659939.
Article22. Bayne CO, Stanley R, Simon P, et al. Effect of capsulotomy on hip stability-a consideration during hip arthroscopy. Am J Orthop (Belle Mead NJ). 2014; 43:160–165. PMID: 24730000.23. Bolia IK, Fagotti L, Briggs KK, Philippon MJ. Midterm outcomes following repair of capsulotomy versus nonrepair in patients undergoing hip arthroscopy for femoroacetabular impingement with labral repair. Arthroscopy. 2019; 35:1828–1834. PMID: 31053455.
Article24. Frank RM, Lee S, Bush-Joseph CA, Kelly BT, Salata MJ, Nho SJ. Improved outcomes after hip arthroscopic surgery in patients undergoing T-capsulotomy with complete repair versus partial repair for femoroacetabular impingement: a comparative matched-pair analysis. Am J Sports Med. 2014; 42:2634–2642. PMID: 25214529.25. Monroe EJ, Chambers CC, Zhang AL. Periportal capsulotomy: a technique for limited violation of the hip capsule during arthroscopy for femoroacetabular impingement. Arthrosc Tech. 2019; 8:e205–e208. PMID: 30906690.26. Weber AE, Neal WH, Mayer EN, et al. Vertical extension of the T-capsulotomy incision in hip arthroscopic surgery does not affect the force required for hip distraction: effect of capsulotomy size, type, and subsequent repair. Am J Sports Med. 2018; 46:3127–3133. PMID: 30307738.
Article27. Forster-Horvath C, Domb BG, Ashberg L, Herzog RF. A method for capsular management and avoidance of iatrogenic instability: minimally invasive capsulotomy in hip arthroscopy. Arthrosc Tech. 2017; 6:e397–e400. PMID: 28580258.
Article28. Harris JD. Capsular management in hip arthroscopy. Clin Sports Med. 2016; 35:373–389. PMID: 27343391.
Article29. Ekhtiari S, de Sa D, Haldane CE, et al. Hip arthroscopic capsulotomy techniques and capsular management strategies: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2017; 25:9–23. PMID: 28120020.
Article30. Chambers CC, Monroe EJ, Flores SE, Borak KR, Zhang AL. Periportal capsulotomy: technique and outcomes for a limited capsulotomy during hip arthroscopy. Arthroscopy. 2019; 35:1120–1127. PMID: 30871902.
Article31. Philippon MJ, Michalski MP, Campbell KJ, et al. An anatomical study of the acetabulum with clinical applications to hip arthroscopy. J Bone Joint Surg Am. 2014; 96:1673–1682. PMID: 25320193.
Article32. Domb BG, Philippon MJ, Giordano BD. Arthroscopic capsulotomy, capsular repair, and capsular plication of the hip: relation to atraumatic instability. Arthroscopy. 2013; 29:162–173. PMID: 22901333.
Article33. Cooper HJ, Walters BL, Rodriguez JA. Anatomy of the hip capsule and pericapsular structures: a cadaveric study. Clin Anat. 2015; 28:665–671. PMID: 25873416.34. Nepple JJ, Smith MV. Biomechanics of the hip capsule and capsule management strategies in hip arthroscopy. Sports Med Arthrosc Rev. 2015; 23:164–168. PMID: 26524549.
Article35. Domb BG, Chaharbakhshi EO, Perets I, Walsh JP, Yuen LC, Ashberg LJ. Patient-reported outcomes of capsular repair versus capsulotomy in patients undergoing hip arthroscopy: minimum 5-year follow-up-a matched comparison study. Arthroscopy. 2018; 34:853–863.e1. PMID: 29373289.
Article36. Domb BG, Stake CE, Finley ZJ, Chen T, Giordano BD. Influence of capsular repair versus unrepaired capsulotomy on 2-year clinical outcomes after arthroscopic hip preservation surgery. Arthroscopy. 2015; 31:643–650. PMID: 25530511.
Article37. Cvetanovich GL, Levy DM, Beck EC, et al. A T-capsulotomy provides increased hip joint visualization compared with an extended interportal capsulotomy. J Hip Preserv Surg. 2019; 6:157–163. PMID: 31660201.
Article38. Ortiz-Declet V, Mu B, Chen AW, et al. Should the capsule be repaired or plicated after hip arthroscopy for labral tears associated with femoroacetabular impingement or instability? A systematic review. Arthroscopy. 2018; 34:303–318. PMID: 28866345.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arthroscopic Control for Safe and Secure Seating of Suspensory Devices for Femoral Fixation in Anterior Cruciate Ligament Reconstruction Using Three Different Techniques
- A New Classification of the Right Portal Vein Using 64 Channel Multi-dectector CT (MDCT)
- Normal Anatomical Variation of the Intrahepatic Portal Vein in Korean
- Robotic-assisted right hepatectomy via anterior approach for intrahepatic cholangiocarcinoma
- Preparation of the Femoral Tunnel through Anteromedial Portal during Arthroscopic Single Incision Anterior Cruciate Ligament Reconstruction
