Single-port robot-assisted radical prostatectomy with the da Vinci SP system: A single surgeon's experience
- Affiliations
-
- 1Department of Urology, Ewha Womans University Seoul Hospital, Seoul, Korea. khkim.uro@gmail.com
- 2Department of Urology, Ewha Womans University Mokdong Hospital, Seoul, Korea.
- KMID: 2471073
- DOI: http://doi.org/10.4111/icu.2020.61.2.173
Abstract
- PURPOSE
To report an initial single-surgeon experience with single-port robot-assisted radical prostatectomy (SP-RARP) using the da Vinci SP surgical system (Intuitive Surgical, USA).
MATERIALS AND METHODS
Between December 2018 and October 2019, a single surgeon performed SP-RARP in 20 patients with prostate cancer. SP-RARP was performed using the conventional approach through an umbilical port with a GelPOINT access system (Applied Medical, USA) and an additional assist port. During surgery, the camera was placed in the 6- or 12-o'clock position, and a traction arm was placed in the counterpart position for upward or downward traction. Clinicopathologic data, perioperative data, and short-term surgical outcomes were analyzed.
RESULTS
Of 20 patients, 45% of patients had pT3 or greater disease and 45% had Gleason grade 4 to 5, respectively. In 11 patients that underwent lymph node dissection, the median number of lymph nodes removed was 19 (interquartile range [IQR], 14-22). Median operative time was 245 minutes (IQR, 200-255), and median console time was 190 minutes (IQR, 165-210). Median blood loss was 200 mL (IQR, 150-300 mL), and there were no intraoperative complications or open conversion. In 10 patients with a follow-up period longer than 3 months, one patient experienced biochemical recurrence, and all patients required 0 to 1 pads per day. Of seven patients that were potent before surgery, four recovered erectile function sufficient for intercourse.
CONCLUSIONS
Our report shows the safety and feasibility of SP-RARP, and that the associated surgical outcomes with short-term follow-up are satisfactory.
Keyword
MeSH Terms
Figure
-
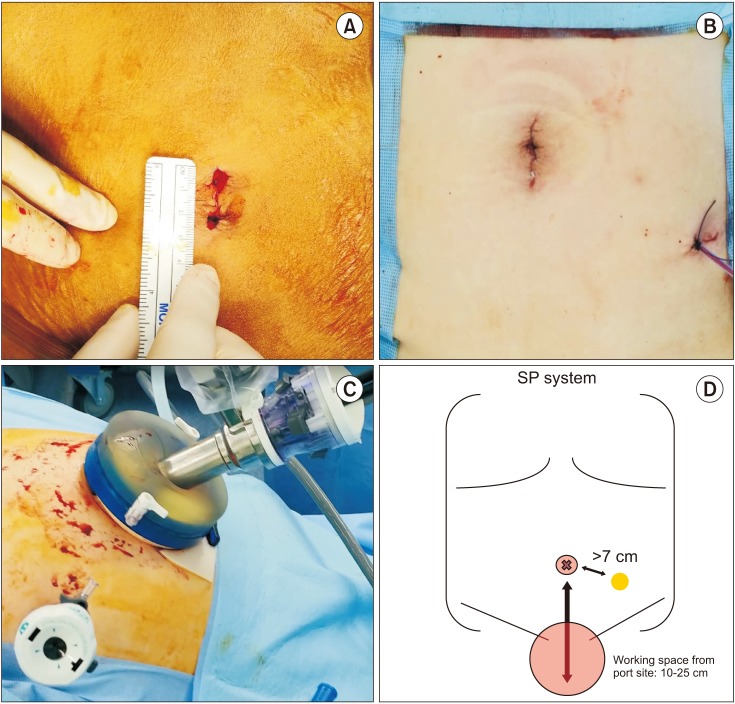
Fig. 1 (A) Umbilical incision for port placement, (B) final incision after surgery, (C) and (D) port placement for single-port robot-assisted radical prostatectomy (SP-RARP). The assist port should be place at least 7 cm from the SP port, and the working space should be within 10 to 25 cm from the SP port for robotic arm triangulation.
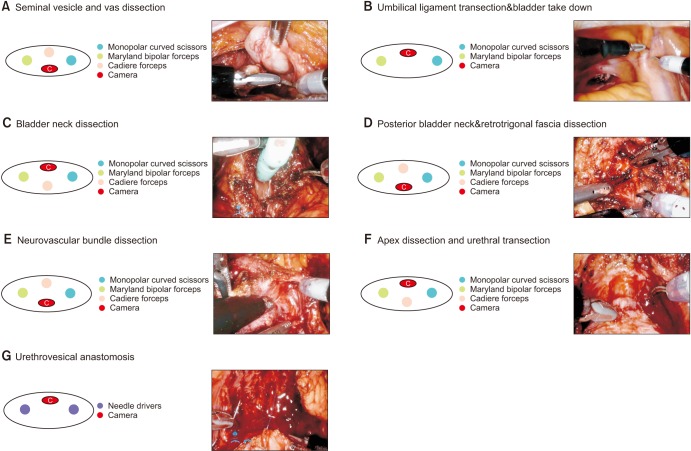
Fig. 2 The single-port robot-assisted radical prostatectomy (SP-RARP) surgical procedures. The camera was placed in the 6-o'clock position during (A) seminal vesicle dissection, (D) posterior bladder neck dissection, and (E) neurovascular bundle dissection with upward traction created by Cadiere forceps in the 12-o'clock position. (B) Umbilical ligament transection, (C) bladder neck transection, (F) apex dissection, and (G) urethrovesical anastomosis were performed with the camera positioned at 12 o'clock.

Fig. 3 (A) Console time and (B) estimated blood loss for single-port robot-assisted radical prostatectomy. PLND, pelvic lymph node dissection; EBL, estimated blood loss.
Reference
-
1. Oberlin DT, Flum AS, Lai JD, Meeks JJ. The effect of minimally invasive prostatectomy on practice patterns of American urologists. Urol Oncol. 2016; 34:255.e1–255.e5.
Article2. Park J, Suh B, Shin DW, Hong JH, Ahn H. Changing patterns of primary treatment in Korean men with prostate cancer over 10 years: a nationwide population based study. Cancer Res Treat. 2016; 48:899–906. PMID: 26511804.
Article3. Ficarra V, Novara G, Rosen RC, Artibani W, Carroll PR, Costello A, et al. Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy. Eur Urol. 2012; 62:405–417. PMID: 22749852.
Article4. Ficarra V, Novara G, Ahlering TE, Costello A, Eastham JA, Graefen M, et al. Systematic review and meta-analysis of studies reporting potency rates after robot-assisted radical prostatectomy. Eur Urol. 2012; 62:418–430. PMID: 22749850.
Article5. Kaouk JH, Goel RK, Haber GP, Crouzet S, Stein RJ. Robotic single-port transumbilical surgery in humans: initial report. BJU Int. 2009; 103:366–369. PMID: 18778353.
Article6. Agarwal DK, Sharma V, Toussi A, Viers BR, Tollefson MK, Gettman MT, et al. Initial experience with da vinci single-port robot-assisted radical prostatectomies. Eur Urol. 2019; 4. 19. DOI: 10.1016/j.eururo.2019.04.001. [Epub].
Article7. Kaouk J, Bertolo R, Eltemamy M, Garisto J. Single-port robot-assisted radical prostatectomy: first clinical experience using the sp surgical system. Urology. 2019; 124:309. PMID: 30367924.
Article8. Kaouk J, Garisto J, Bertolo R. Robotic urologic surgical interventions performed with the single port dedicated platform: first clinical investigation. Eur Urol. 2019; 75:684–691. PMID: 30522914.
Article9. Bertolo R, Garisto J, Gettman M, Kaouk J. Novel system for robotic single-port surgery: feasibility and state of the art in urology. Eur Urol Focus. 2018; 4:669–673. PMID: 29914841.
Article10. Nelson RJ, Chavali JSS, Yerram N, Babbar P, Kaouk JH. Current status of robotic single-port surgery. Urol Ann. 2017; 9:217–222. PMID: 28794585.
Article11. Dobbs RW, Halgrimson WR, Madueke I, Vigneswaran HT, Wilson JO, Crivellaro S. Single-port robot-assisted laparoscopic radical prostatectomy: initial experience and technique with the da Vinci(®) SP platform. BJU Int. 2019; 124:1022–1027. PMID: 31301693.12. Ng CF, Chan ESY, Teoh JYC. The use of the da Vinci SP system for retzius-sparing radical prostatectomy in cadaveric model. Urology. 2019; 125:260. PMID: 30580003.
Article13. Kaouk J, Valero R, Sawczyn G, Garisto J. Extraperitoneal single-port robot-assisted radical prostatectomy: initial experience and description of technique. BJU Int. 2019; 8. 06. DOI: 10.1111/bju.14885. [Epub].
Article14. Ng CF, Teoh JY, Chiu PK, Yee CH, Chan CK, Hou SS, et al. Robot-assisted single-port radical prostatectomy: a phase 1 clinical study. Int J Urol. 2019; 26:878–883. PMID: 31257704.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single-port robot-assisted prosthetic breast reconstruction with the da Vinci SP Surgical System: first clinical report
- Da Vinci SP Single-Port Robotic Surgery in Gynecologic Tumors: Single Surgeon’s Initial Experience with 100 Cases
- Robot-assisted laparoendoscopic single-site upper urinary tract surgery with da Vinci Xi surgical system: Initial experience
- Comparison of intraoperative and short-term postoperative outcomes between robot-assisted laparoscopic multi-port pyeloplasty using the da Vinci Si system and single-port pyeloplasty using the da Vinci SP system in children
- Pure single-site robot-assisted pyeloplasty with the da Vinci SP surgical system: Initial experience
