Cauda Equina Syndrome after Percutaneous Balloon Kyphoplasty for Pathologic Compression Fracture
- Affiliations
-
- 1Department of Orthopedic Surgery, College of Medicine, Inha University, Incheon, Korea. chokj@inha.ac.kr
- KMID: 2470774
- DOI: http://doi.org/10.4055/jkoa.2020.55.1.90
Abstract
- Percutaneous balloon kyphoplasty is an option for pain relief in pathological vertebral compression fractures. Complications related to cement leakage through cortical defects have been reported. On the other hand, dural compression due to retropulsion of the tumor mass is rarely reported. The authors report a case of a 65-year female patient who had cauda equina syndrome after a percutaneous balloon kyphoplasty in a pathological vertebral fracture, even though epidural compression were not found prior to surgery. Magnetic resonance imaging revealed retropulsion of the tumor mass into the spinal canal through the disrupted posterior vertebral cortex.
MeSH Terms
Figure
-
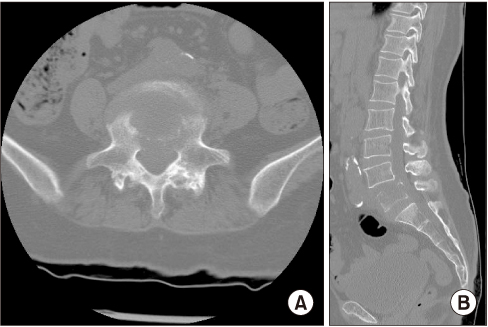
Figure 1 Sagittal (A), axial (B) computed tomography scan showed pathologic fracture with osteolysis at L5 vertebral body, suggesting a metastatic tumor.
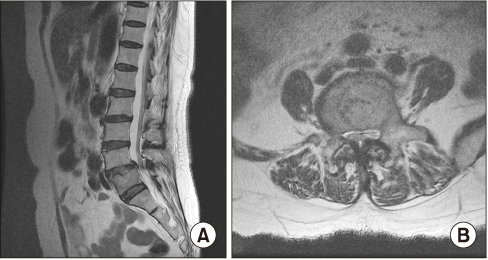
Figure 2 Sagittal T2-weighted (A), axial T2-weighted (B) spinal magnetic resonance imaging show a contrast-enhancing mass at L5 vertebral body.
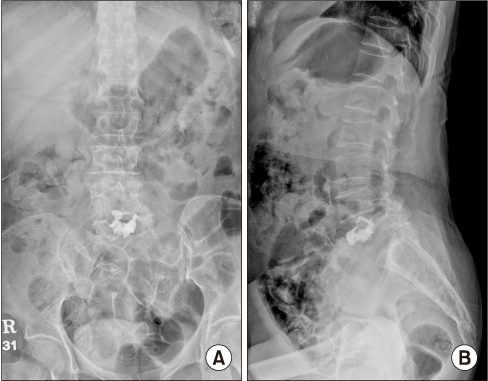
Figure 3 Lumbar spine anteroposterior (A), lateral (B) radiographs showed cement within V5 vertebral body with cement leakage to L4–5 disc space.
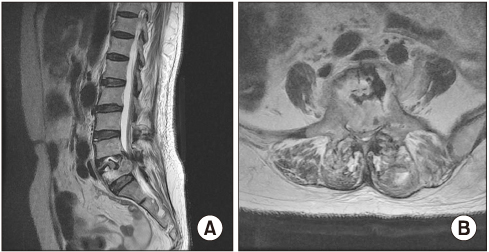
Figure 4 Sagittal T2-weighted (A), axial T2-weighted (B) magnetic resonance imaging show retropulsion of neoplastic tissue with significant epidural compression of dural sac of L5 body.
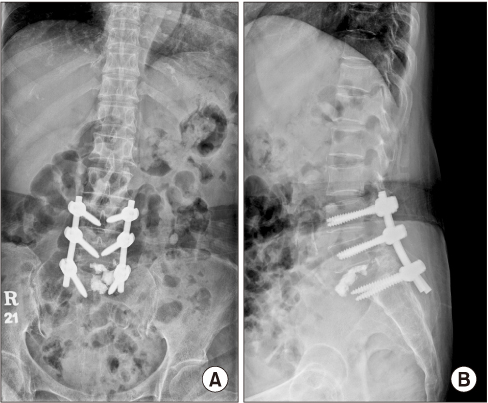
Figure 5 Lumbar spine anteroposterior (A), lateral (B) radiographs showing pedicle screw instrumentation in L45S1.
Reference
-
1. Fourney DR, Schomer DF, Nader R, et al. Percutaneous vertebroplasty and kyphoplasty for painful vertebral body fractures in cancer patients. J Neurosurg. 2003; 98:1 Suppl. 21–30.
Article2. Gokaslan ZL, York JE, Walsh GL, et al. Transthoracic vertebrectomy for metastatic spinal tumors. J Neurosurg. 1998; 89:599–609.
Article3. Pilitsis JG, Rengachary SS. The role of vertebroplasty in metastatic spinal disease. Neurosurg Focus. 2001; 11:e9.
Article4. Galibert P, Deramond H, Rosat P, Le Gars D. [Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty]. Neurochirurgie. 1987; 33:166–168. French.5. Martin JB, Jean B, Sugiu K, et al. Vertebroplasty: clinical experience and follow-up results. Bone. 1999; 25:2 Suppl. 11S–15S.
Article6. Ratliff J, Nguyen T, Heiss J. Root and spinal cord compression from methylmethacrylate vertebroplasty. Spine (Phila Pa 1976). 2001; 26:E300–E302.
Article7. Murphy KJ, Deramond H. Percutaneous vertebroplasty in benign and malignant disease. Neuroimaging Clin N Am. 2000; 10:535–545.8. Lieberman IH, Dudeney S, Reinhardt MK, Bell G. Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. Spine (Phila Pa 1976). 2001; 26:1631–1638.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Study of Electrodiagnostic Changes after Decompression of Chronic Cauda equina compression in dogs
- Causes and Clinical Manifestations of Cauda Equina Syndrome
- Cavernous Hemangioma of the Cauda Equina
- Single-Balloon Kyphoplasty in Osteoporotic Vertebral Compression Fractures : Far-Lateral Extrapedicular Approach
- Cauda Equina Syndrome after Laminectomy of Lumbar Spine with Application of Autogenous Free Fat Graft: A Case Report
