Tension Band Wiring Technique for Distal Radius Fracture with a Volar Articular Marginal Fragment: Technical Note
- Affiliations
-
- 1Department of Orthopedic Surgery, MS Jaegeon Hospital, Daegu, Korea.
- 2Department of Orthopedic Surgery, Korea University Guro Hospital, Seoul, Korea.
- 3Department of Orthopedic Surgery, The Catholic University of Korea, Uijeongbu St. Mary's Hospital, Uijeongbu, Korea. medicyoung1979@gmail.com
- KMID: 2468673
- DOI: http://doi.org/10.12671/jkfs.2020.33.1.38
Abstract
- Most distal radius fractures are currently being treated with anterior plating using anatomical precontoured locking compression plates via the anterior approach. However, it is difficult to fix the volar articular marginal fragment because these anatomical plates should be placed proximally to the watershed line. There were just a few methods of fixation for this fragment on medical literature. Herein, we introduced a tension band wiring technique for fixation of a volar articular marginal fragment in the distal radius.
MeSH Terms
Figure
-
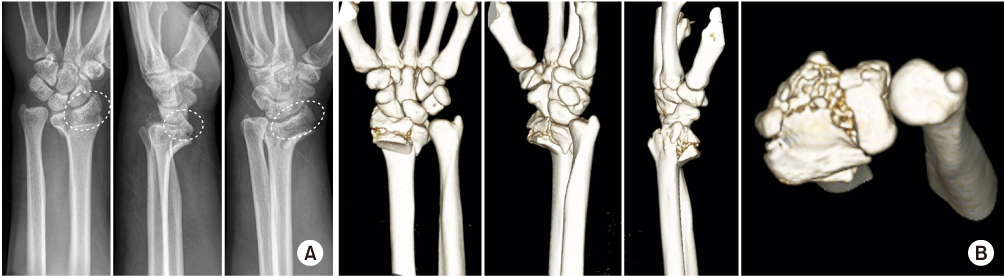
Fig. 1 (A) Volar articular marginal fragment (circles with the dotted line) with a comminuted metaphyseal fracture of the distal radius on plain radiography. (B) Three-dimensional computed tomography scan also shows the volar articular marginal fragment.
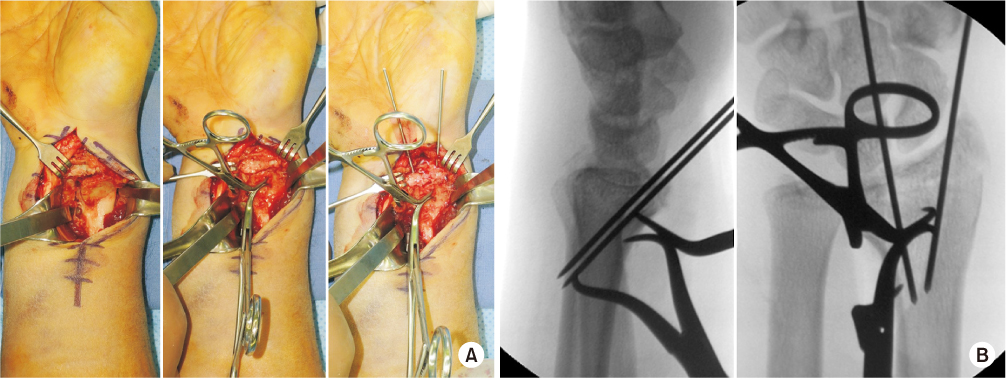
Fig. 2 (A) Two K-wires were inserted from the distal edge of the volar articular marginal fragment to the posterior cortex proximally and posteriorly after reduction with pointed forceps through the modified Henry approach. (B) The position of two K-wires was checked on the anteroposterior and lateral view of the C-arm image.
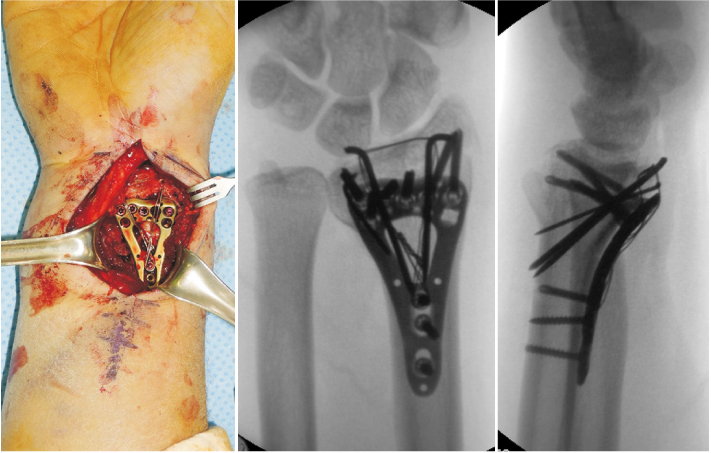
Fig. 3 Tension band wiring for the volar articular marginal fragment after plating.
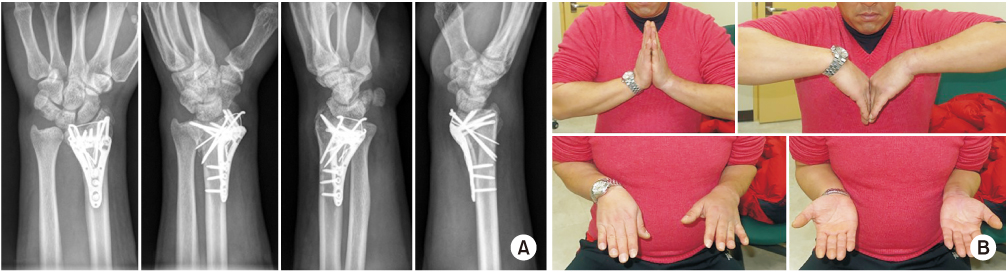
Fig. 4 Radiologic union (A) and near full fuctional recovery (B) were achieved at postoperative 6 weeks.

Fig. 5 (A) The simple volar articular marginal fragment of the distal radius on plain radiography. (B) Three-dimensional computed tomography scan also shows more clearly the volar articular marginal fragment.
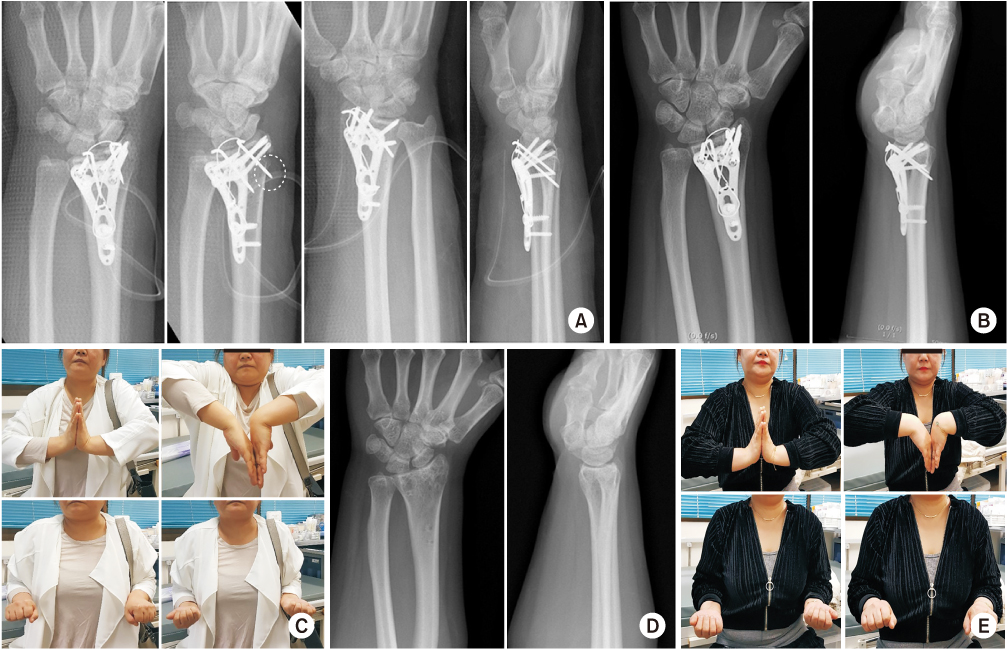
Fig. 6 (A) Immediate postoperative radiograph. Protrusion of the K-wire was seen on the oblique view (circle with the dotted line). (B) Complete union was seen on the postoperative 1-year X-ray. (C) Deficit of wrist flexion still remained due to protrusion of the K-wire at postoperative 1-year follow up. (D) Postoperative X-ray after implant removal. (E) The deficit of wrist flexion was full recovered after removal of the implant.
Reference
-
1. Conti Mica MA, Bindra R, Moran SL. Anatomic considerations when performing the modified Henry approach for exposure of distal radius fractures. J Orthop. 2017; 14:104–107.
Article2. Orbay J. Volar plate fixation of distal radius fractures. Hand Clin. 2005; 21:347–354.
Article3. Chin KR, Jupiter JB. Wire-loop fixation of volar displaced osteochondral fractures of the distal radius. J Hand Surg Am. 1999; 24:525–533.
Article4. Schumer ED, Leslie BM. Fragment-specific fixation of distal radius fractures using the Trimed device. Tech Hand Up Extrem Surg. 2005; 9:74–83.
Article5. Katznelson A, Volpin G, Lin E. Tension band wiring for fixation of comminuted fractures of the distal radius. Injury. 1980; 12:239–242.
Article6. van Aaken J, Beaulieu JY, Della Santa D, Kibbel O, Fusetti C. High rate of complications associated with extrafocal kirschner wire pinning for distal radius fractures. Chir Main. 2008; 27:160–166.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Clinical Results of Tension Band Wiring
- Tension band wiring and Modified tension band wiring in the Operative Treatment of Patella Fracture
- Modified Tension Band Wiring Combined with Anti-Gliding Loop Augmentation Technique for the Treatment of Comminuted Patellar Fracture: Technical Note and Report of Early Results: Technical Note
- Tension Band Wiring with Anchoring Screw in Medial Malleolar Fracture
- Operative Treatment of patellar Fractures
