A Case of Congenital Nasal Pyriform Aperture Stenosis
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Eulji University Medical Center, Eulji University School of Medicine, Daejeon, Korea. mschoi@eulji.ac.kr
- 2Department of Radiology, Eulji University Medical Center, Eulji University School of Medicine, Daejeon, Korea.
- KMID: 2465544
- DOI: http://doi.org/10.18787/jr.2019.26.2.117
Abstract
- Congenital nasal pyriform aperture stenosis (CNPAS) is a rare cause of upper airway obstruction in the newborn. This affliction is due to bony overgrowth of the nasal process of the maxilla. CNPAS is diagnosed clinically and confirmed with CT scan. Patients can be managed conservatively or surgically. In this report, a male neonate had respiratory distress, cyclic cyanosis, and apnea after delivery. The patient underwent surgical correction of pyriform stenosis with a transnasal approach. During follow up, the patient showed recurred respiratory distress and cyanosis. Revision operation was necessary to reduce the bony inferior turbinate and pyriform aperture. CNPAS should be suspected in newborns with clinical signs of severe nasal obstruction associated with difficulty passing a small catheter through the anterior nares.
MeSH Terms
Figure
-
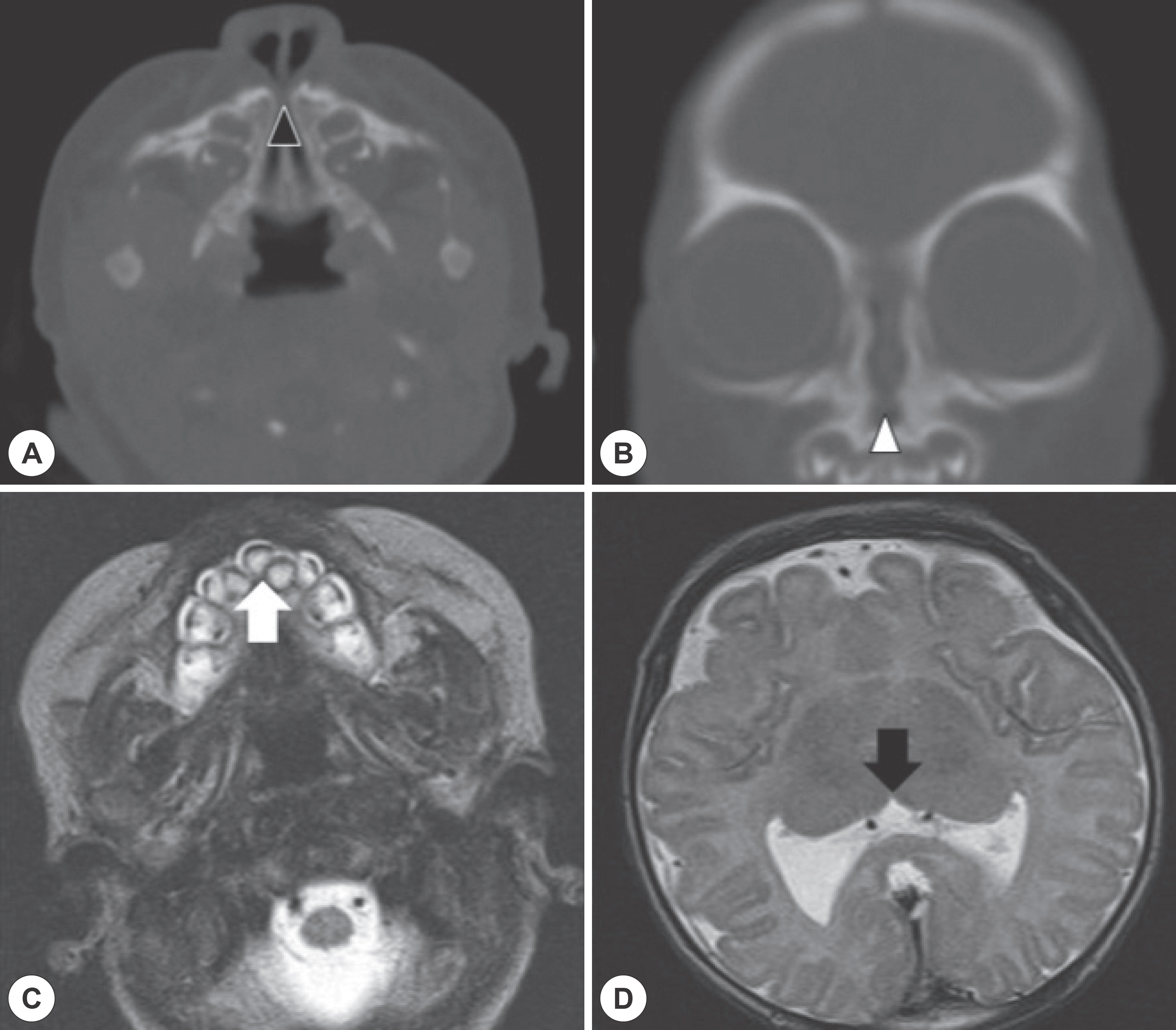
Fig. 1. Radiology of congenital nasal pyriform aperture stenosis. (A) Axial view of facial CT image, note that narrow width of nasal pyr-iform aperture. a black arrowhead indicates nasal pyriform aperture (B) Coronal view of facial CT image, note that narrow width of nasal pyriform aperture. a white arrowhead indicates nasal pyriform aperture (C) MRI demonstrates associated anomalies with con-genital nasal pyriform aperture stenosis, a white arrow indicates a single median maxillary central incisor and (D) MRI demonstrates as-sociated anomalies with congenital nasal pyriform aperture stenosis, a black arrow indicates a monoventricle which can be seen in lobar holoprosencephaly.
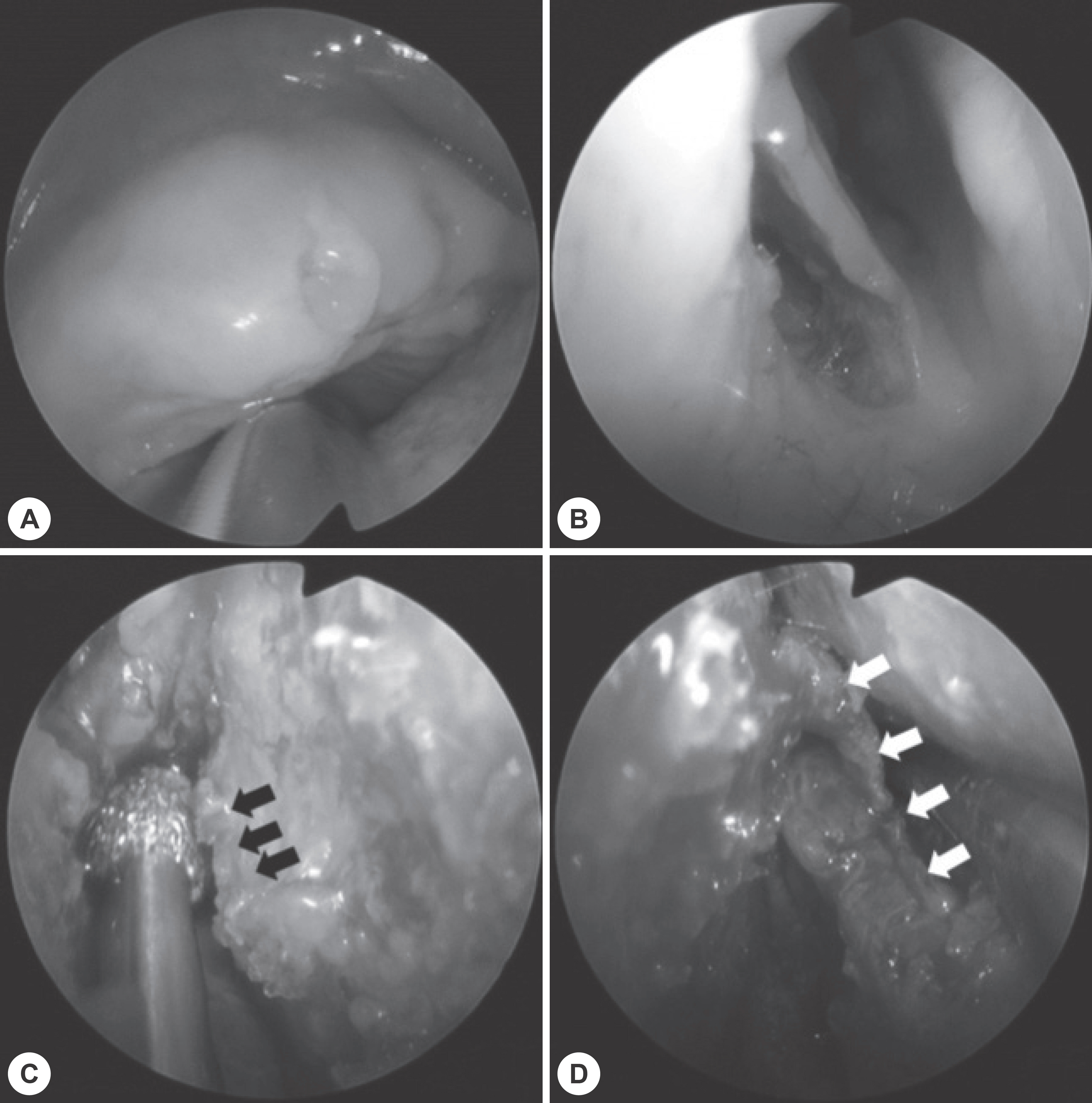
Fig. 2. Intraoperative findings of pyriform aperture stenosis. A: A single median maxillary central incisor was seen in upper gingiva. B: Making an incision on the nasal vestibular skin above pyriform aperture. C: Lt. nasal process of the maxilla was identified and drilled out. Black arrows indicate remnant nasal process of the maxilla. D: Left inferior turbinate was identified and drilled out. White arrows indicate attachment of inferior turbinate on the lateral wall in the right side.

Fig. 3. Nostrils of newborn. A, B: Nasopharyngoscope images, which were taken 17days after first operation. Narrow pyriform aperture and hypertrophied inferior turbinates were seen. C, D: Nasopharyngoscope images, which were taken 40days after second operation. Note that widened anterior nares.
Reference
-
References
1. Syed KA, Raja K, Kolethekkat AA, Varghese AM, Al Abri R, Ku-rine M. Congenital midnasal stenosis–A novel technique for management. Int J Pediatr Otorhinolaryngol. 2016; 87:117–20.2. Douglas B. The relief of vestibular nasal obstruction by partial resection of the nasal process of the superior maxilla. Plast Reconstr Surg. 1952; 9(1):42–51.3. Brown OE, Myer CM 3rd, Manning SC. Congenital nasal pyriform aperture stenosis. Layrngoscope. 1989; 99(1):86–91.
Article4. Levison J, Neas K, Wilson M, Cooper P, Wojtulewicz J. Neonatal nasal obstruction and a single maxillary central incisor. J Paediatr Child Health. 2005; 41(7):308–1.
Article5. Visvanathan V, Wynne DM. Congenital nasal pyriform aperture stenosis: a report of 10 cases and literature review. Int J Pediatr Otorhinolaryngology. 2012; 76(1):28–30.
Article6. Moreddu E, Le Treut-Gay C, Triglia JM, Nicollas R. Congenital nasal pyriform aperture stenosis: Elaboration of a management algorithm from 25 years of experience. Int J Pediatr Otorhinolaryngolo-gy. 2016; 83:7–11.
Article7. Moreddu E, Pereira J, Vaz R, Lena G, Triglia JM, Nicollas R. Combined endonasal and neurosurgical resection of a congenital teratoma with pharyngeal, intracranial and orbital extension: Case report, surgical technique and review of the literature. Int J Pediatr Otorhinolaryngol. 2015; 79(12):1991–4.
Article8. Bachelard-Serra M, Chau C, Farinetti A, Roman S, Triglia JM, Nicollas R. Prenatal diagnosis of congenital dacryocystocle, Int J Pediatr Otorhinolaryngol. 2013; 77(5):847–9.9. Wormald R, Hinton-Bayre A, Bumbak P, Vijayasekaran S. Congenital nasal pyriform aperture stenosis 5.7 mm or less is associated with surgical intervention: A pooled case series, Int J Pediatr Otorhinolaryngology. 2015; 79(11):1802–5.10. Belden CJ, Mancuso AA, Schmalfuss IM. CT features of congenital nasal pyriform aperture stenosis: initial experience. Radiology. 1999; 213(2):495–501.11. Sesenna E, Leporati M, Brevi B, Oretti G, Ferri A. Congenital nasal pyriform aperture stenosis: diagnosis and management. Ital J Pediatr. 2012 26; 38:28.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Congenital Nasal Pyriform Aperture Stenosis
- A Case of Respiratory Difficulty Due to Congenital Tracheal Calcification and Nasal Pyriform Aperture Stenosis
- A Case of Congenital Nasal Piriform Aperture Stenosis (CNPAS)
- Correction of Depressed Nasal Base and Piriform Aperture Using Polyethylene Implants
- Rare Cleft of the Nose
