Qualitative Analysis on Magnetic Resonance Imaging for Preoperative Evaluation of Chronic Lateral Ankle Ligament Injury
- Affiliations
-
- 1Department of Radiology, Konkuk University School of Medicine, Seoul, Korea. kimnr001@gmail.com
- 2Department of Orthopedics, Konkuk University School of Medicine, Seoul, Korea.
- KMID: 2464911
- DOI: http://doi.org/10.3348/jksr.2019.80.6.1121
Abstract
- PURPOSE
To compare the MRI findings of anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) injuries in chronic lateral ankle instability (CLAI) between surgical treatment groups.
MATERIALS AND METHODS
Fifty-two patients with CLAI were divided into the modified Broström procedure (MBP) (n = 31) and lateral ankle ligament reconstruction (LAR) (n = 21) groups. T2-weighted MRI findings between the groups were compared for caliber change, slope, signal intensity, and thickness measurements of the ligaments. Additionally, the talar tilt angles were measured on stress radiographs.
RESULTS
The injured ATFL (p = 0.002 vs. p = 0.001) and CFL (p = 0.008 vs. p = 0.039) were more commonly scarce or thin and had decreased slopes in the LAR group. The mean thickness of ATFL (P = 0.002) and CFL (p = 0.002) was 1.1 ± 0.9 mm and 1.3 ± 0.8 mm, respectively, in the LAR group and 2.2 ± 1.3 mm and 2.1 ± 0.9 mm, respectively, in the MBP group. The mean talar tilt angle was greater in the LAR group (13.4 ± 3.9°) than in the MBP group (9.5 ± 3.8°) (p = 0.001).
CONCLUSION
A qualitative analysis of the ligaments on MRI is valuable in selecting the surgical method.
MeSH Terms
Figure
-
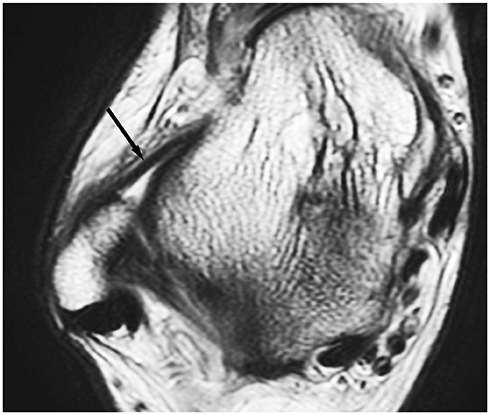
Fig. 1 A 35-year-old woman with chronic ankle pain. The anterior talofibular ligament is well-visualized on axial T2-weighted image. The uninjured ligament is of uniform thickness and low T2 signal intensity (arrow).
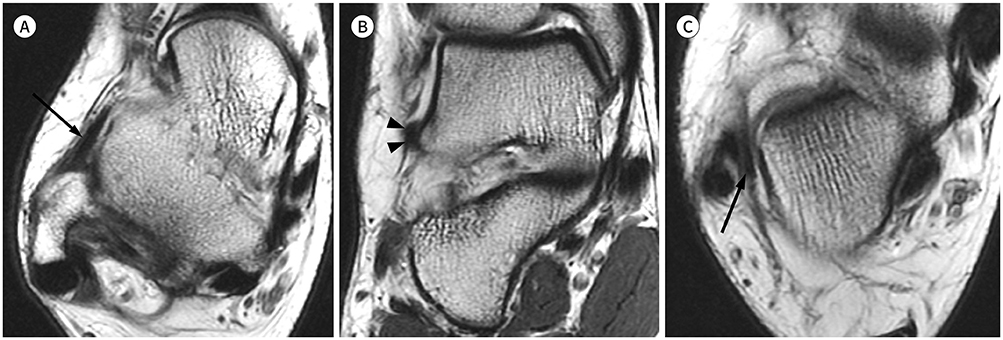
Fig. 2 A 26-year-old woman who underwent the modified Broström procedure for the treatment of chronic lateral ankle instability. The talar tilt angle on ankle inversion stress radiography was 9°. A. Axial T2-weighted image shows diffuse thickening of the ATFL with low signal intensity and normal slope (arrow). B. Coronal T2-weighted image reveals a thickened ATFL (arrowheads). C. Axial T2-weighted image shows mild thickening of the calcaneofibular ligament with low signal intensity and normal slope (arrow). ATFL = anterior talofibular ligament
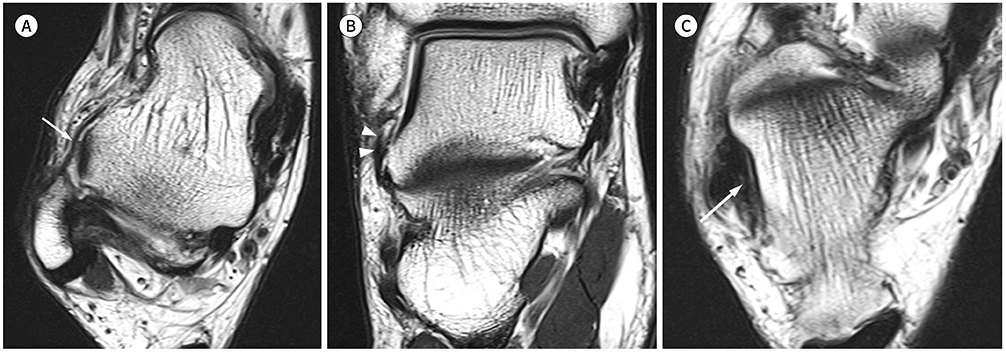
Fig. 3 A 38-year-old man who underwent lateral ankle ligament reconstruction for the treatment of chronic lateral ankle instability. The talar tilt angle on ankle inversion stress radiography was 16°. A. The injured ATFL has a thin and wavy appearance with low signal intensity (arrow) on an axial T2-weighted image. B. Coronal T2-weighted image reveals a thinned ATFL (arrowheads). C. Axial T2-weighted image shows irregular thinning of the calcaneofibular ligament with low signal intensity and decreased slope (arrow). ATFL = anterior talofibular ligament
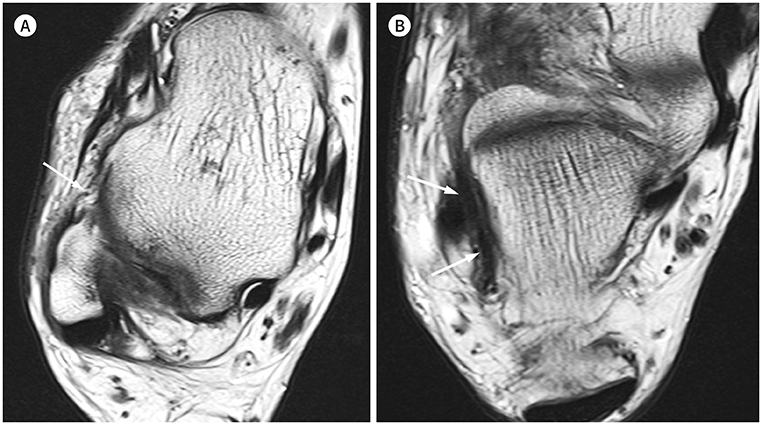
Fig. 4 A 55-year-old man who underwent lateral ankle ligament reconstruction for the treatment of chronic lateral ankle instability. The talar tilt angle on ankle inversion stress radiography was 15°. A. Axial T2-weighted image demonstrates a markedly thin and wavy anterior talofibular ligament with focal discontinuity (arrow). B. Axial T2-weighted image shows irregular thickening of the calcaneofibular ligament with low signal intensity and decreased slope (arrows).
Reference
-
1. Waterman BR, Owens BD, Davey S, Zacchilli MA, Belmont PJ Jr. The epidemiology of ankle sprains in the United States. J Bone Joint Surg Am. 2010; 92:2279–2284.2. Bridgman SA, Clement D, Downing A, Walley G, Phair I, Maffulli N. Population based epidemiology of ankle sprains attending accident and emergency units in the West Midlands of England, and a survey of UK practice for severe ankle sprains. Emerg Med J. 2003; 20:508–510.3. Brooks SC, Potter BT, Rainey JB. Treatment for partial tears of the lateral ligament of the ankle: a prospective trial. Br Med J (Clin Res Ed). 1981; 282:606–607.4. Safran MR, Benedetti RS, Bartolozzi AR 3rd, Mandelbaum BR. Lateral ankle sprains: a comprehensive review: part 1: etiology, pathoanatomy, histopathogenesis, and diagnosis. Med Sci Sports Exerc. 1999; 31:S429–S437.5. O'Loughlin PF, Murawski CD, Egan C, Kennedy JG. Ankle instability in sports. Phys Sportsmed. 2009; 37:93–103.6. Staples OS. Ruptures of the fibular collateral ligaments of the ankle. Result study of immediate surgical treatment. J Bone Joint Surg Am. 1975; 57:101–107.7. Balduini FC, Vegso JJ, Torg JS, Torg E. Management and rehabilitation of ligamentous injuries to the ankle. Sports Med. 1987; 4:364–380.8. Van den Bekerom MP, Oostra RJ, Golanó P, Van Dijk CN. The anatomy in relation to injury of the lateral collateral ligaments of the ankle: a current concepts review. Clin Anat. 2008; 21:619–626.9. Hertel J. Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. J Athl Train. 2002; 37:364–375.10. Trc T, Handl M, Havlas V. The anterior talo-fibular ligament reconstruction in surgical treatment of chronic lateral ankle instability. Int Orthop. 2010; 34:991–996.11. Matheny LM, Johnson NS, Liechti DJ, Clanton TO. Activity level and function after lateral ankle ligament repair versus reconstruction. Am J Sports Med. 2016; 44:1301–1308.12. Dierckman BD, Ferkel RD. Anatomic reconstruction with a semitendinosus allograft for chronic lateral ankle instability. Am J Sports Med. 2015; 43:1941–1950.13. Kanamoto T, Shiozaki Y, Tanaka Y, Yonetani Y, Horibe S. The use of MRI in pre-operative evaluation of anterior talofibular ligament in chronic ankle instability. Bone Joint Res. 2014; 3:241–245.14. Jung HG, Kim NR, Kim TH, Eom JS, Lee DO. Magnetic resonance imaging and stress radiography in chronic lateral ankle instability. Foot Ankle Int. 2017; 38:621–626.15. Gould N, Seligson D, Gassman J. Early and late repair of lateral ligament of the ankle. Foot Ankle. 1980; 1:84–89.16. Jung HG, Kim TH, Park JY, Bae EJ. Anatomic reconstruction of the anterior talofibular and calcaneofibular ligaments using a semitendinosus tendon allograft and interference screws. Knee Surg Sports Traumatol Arthrosc. 2012; 20:1432–1437.17. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994; 15:349–353.18. Karlsson J, Peterson L. Evaluation of ankle joint function: the use of a scoring scale. The Foot. 1991; 1:15–19.19. Dimmick S, Kennedy D, Daunt N. Evaluation of thickness and appearance of anterior talofibular and calcaneofibular ligaments in normal versus abnormal ankles with MRI. J Med Imaging Radiat Oncol. 2008; 52:559–563.20. Choo HJ, Lee SJ, Kim DW, Jeong HW, Gwak H. Multibanded anterior talofibular ligaments in normal ankles and sprained ankles using 3D isotropic proton density-weighted fast spin-echo MRI sequence. AJR Am J Roentgenol. 2014; 202:W87–W94.21. Broström L. Sprained ankles. VI. Surgical treatment of "chronic" ligament ruptures. Acta Chir Scand. 1966; 132:551–565.22. Clanton TO, Viens NA, Campbell KJ, Laprade RF, Wijdicks CA. Anterior talofibular ligament ruptures, part 2: biomechanical comparison of anterior talofibular ligament reconstruction using semitendinosus allografts with the intact ligament. Am J Sports Med. 2014; 42:412–416.23. Takao M, Innami K, Matsushita T, Uchio Y, Ochi M. Arthroscopic and magnetic resonance image appearance and reconstruction of the anterior talofibular ligament in cases of apparent functional ankle instability. Am J Sports Med. 2008; 36:1542–1547.24. Raatikainen T, Putkonen M, Puranen J. Arthrography, clinical examination, and stress radiograph in the diagnosis of acute injury to the lateral ligaments of the ankle. Am J Sports Med. 1992; 20:2–6.25. Fujii T, Luo ZP, Kitaoka HB, An KN. The manual stress test may not be sufficient to differentiate ankle ligament injuries. Clin Biomech (Bristol, Avon). 2000; 15:619–623.26. Frost SC, Amendola A. Is stress radiography necessary in the diagnosis of acute or chronic ankle instability? Clin J Sport Med. 1999; 9:40–45.27. Lee KM, Chung CY, Kwon SS, Chung MK, Won SH, Lee SY, et al. Relationship between stress ankle radiographs and injured ligaments on MRI. Skeletal Radiol. 2013; 42:1537–1542.28. Chandnani VP, Harper MT, Ficke JR, Gagliardi JA, Rolling L, Christensen KP, et al. Chronic ankle instability: evaluation with MR arthrography, MR imaging, and stress radiography. Radiology. 1994; 192:189–194.29. Oae K, Takao M, Uchio Y, Ochi M. Evaluation of anterior talofibular ligament injury with stress radiography, ultrasonography and MR imaging. Skeletal Radiol. 2010; 39:41–47.30. Park HJ, Cha SD, Kim SS, Rho MH, Kwag HJ, Park NH, et al. Accuracy of MRI findings in chronic lateral ankle ligament injury: comparison with surgical findings. Clin Radiol. 2012; 67:313–318.31. Rosenberg ZS, Beltran J, Bencardino JT. From the RSNA Refresher Courses. Radiological Society of North America. MR imaging of the ankle and foot. Radiographics. 2000; 20(Spec No):S153–S179.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis of Lateral Ankle Ligament Injury in the Evaluation of Chronic Lateral Ankle Instability
- Deltoid Ligament and Tibiofibular Syndesmosis Injury in Chronic Lateral Ankle Instability: Magnetic Resonance Imaging Evaluation at 3T and Comparison with Arthroscopy
- Are Magnetic Resonance Imaging Findings of Ankle Instability Always Correlated with Operative and Physical Examination Findings?
- Injury of the ligaments of the knee: magnetic resonance evaluation
- Chronic Lateral Ankle Instability
