Locating the Instant Center of Rotation in the Subaxial Cervical Spine with Biplanar Fluoroscopy during In Vivo Dynamic Flexion-Extension
- Affiliations
-
- 1Department of Orthopedic Surgery, Chung-Ang University College of Medicine, Seoul, Korea. ksong70@cau.ac.kr
- 2Department of Neurosurgery, Chung-Ang University College of Medicine, Seoul, Korea.
- 3Department of Bioengineering, Chung-Ang University College of Engineering, Seoul, Korea.
- KMID: 2462544
- DOI: http://doi.org/10.4055/cios.2019.11.4.482
Abstract
- BACKGROUND
Recently, biplanar fluoroscopy is used to evaluate the cervical kinematics, especially to locate the instant center of rotation (ICR) during in vivo motion. This study aims to ascertain the ICR at each cervical segment in the sagittal plane during dynamic motion and assess the differences from previous studies.
METHODS
While three healthy subjects were performing full flexion-extension, two oblique views aligned horizontally and angled at approximately 55° were obtained by biplanar fluoroscopy. The minimum degree to detect significant movement in a helical axis model was set at 2°, and anterior-posterior and superior-inferior locations of each ICR were defined. To evaluate the possible distribution area and overlapping area of the ICR with disc space, we drew a circle by using the calculated distance between each coordination and the mean coordination of ICR as the radius.
RESULTS
During flexion-extension motion, the mean superior-inferior location of the ICR became progressively more superior, except the C5-6 segment (p = 0.015), and the mean anterior-posterior location of the ICR became progressively more anterior without exception from C2-3 to C6-7 segments, but anterior-posterior ICR locations were not significantly different among segments. The overlapping area with the distribution circle of ICR was mainly located in the posterior half in the C3-4 segment, but the overlapping area was about 80% of the total disc space in C4-5 and C6-7 segments. The overlapping was more noticeable in the lower cervical segments after exclusion of the outlier data of the C5-6 segment in subject 1.
CONCLUSIONS
The ICR in the cervical spine showed a trend of moving progressively more superiorly and anteriorly and the disc space overlapping the distribution circle of ICR increased along the lower motion segments except the C5-6 segment. These findings could provide a good basis for level-specific cervical arthroplasty designs.
Keyword
Figure
-

Fig. 1 Biplanar fluoroscopic images aligned horizontally and angled at approximately 55° were collected from a system composed of two focal-spot radiograph tubes (KMC–1400ST; COMED Technologies Inc., Gwangju, Korea).
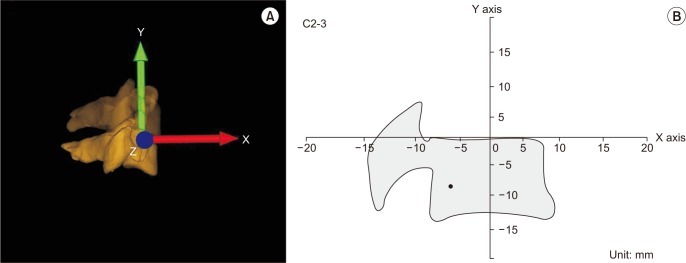
Fig. 2 (A) Three-dimensional reconstruction of the cervical spine from biplanar fluoroscopic projection. The arrow to superior direction represents Y axis; anterior, X axis; horizontal, Z axis. (B) The location of instant center of rotation at the C2–3 segment was calculated by using the (X, Y) coordinate system.
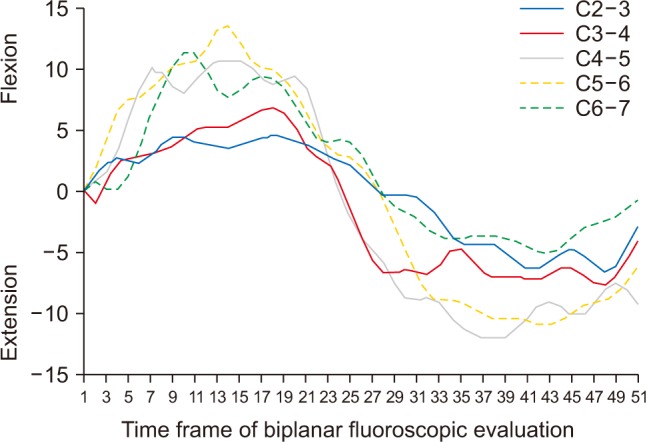
Fig. 3 The overall range of motion in subaxial cervical segments. Positive values mean flexion and negative values mean extension. The greater range of motion was observed in the C4–5 and C5–6 segments.
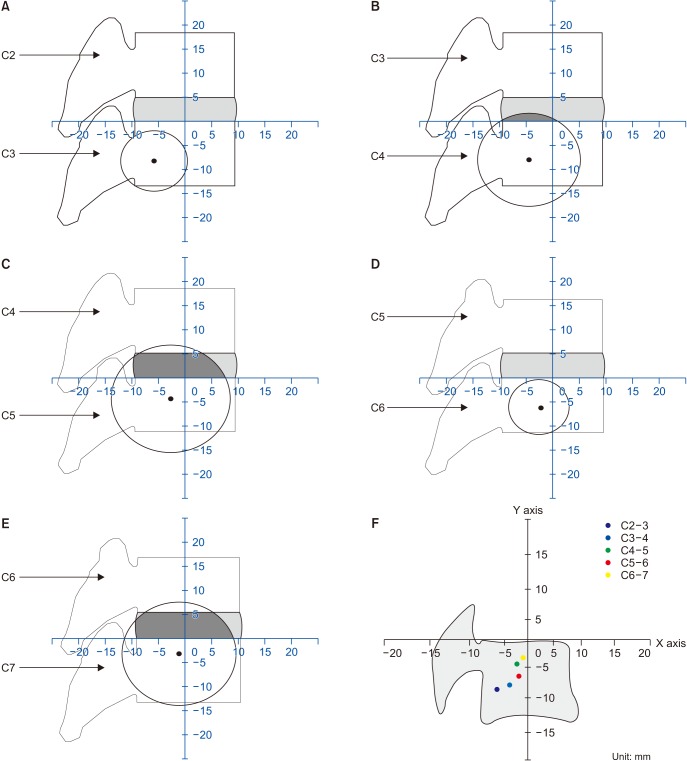
Fig. 4 (A) The radius of circle was measured as 6.3 mm. There was no overlapping area between the circle and intervertebral space in C2–3 segment. (B) The radius of circle was measured as 9.7 mm. The overlapping area was located in the posterior half of intervertebral space in C3–4 segment. (C) The radius of circle was measured as 11.2 mm. The overall posterior area and half of anterior intervertebral space was overlapped by the distribution circle in C4–5 segment. (D) The radius of circle was measured as 5.7 mm. There was no overlapping area between the circle and intervertebral space in C5–6 as in C2–3 segment. (E) The radius of circle was measured as 10.8 mm. The overall intervertebral space was overlapped by the distribution circle in C6–7 as in C4–5 segment. (F) The overall locations of ICR showed a trend of moving progressively superiorly and anteriorly in the lower cervical segments except in C5–6 segment.
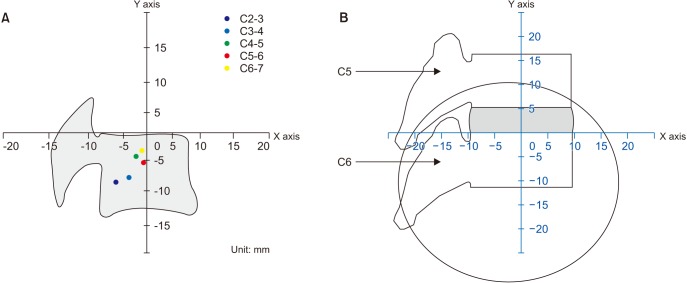
Fig. 5 (A) The location of instant center of rotation of C5–6 segment was changed more superiorly and anteriorly after exclusion of the values of C5–6 segment in subject 1. (B) The overall intervertebral space was overlapped by the distribution circle after exclusion of the values of subject 1.
Reference
-
1. Galbusera F, Bellini CM, Brayda-Bruno M, Fornari M. Biomechanical studies on cervical total disc arthroplasty: a literature review. Clin Biomech (Bristol, Avon). 2008; 23(9):1095–1104.
Article2. Heller JG, Sasso RC, Papadopoulos SM, et al. Comparison of BRYAN cervical disc arthroplasty with anterior cervical decompression and fusion: clinical and radiographic results of a randomized, controlled, clinical trial. Spine (Phila Pa 1976). 2009; 34(2):101–107. PMID: 19112337.3. Powell JW, Sasso RC, Metcalf NH, Anderson PA, Hipp JA. Quality of spinal motion with cervical disk arthroplasty: computer-aided radiographic analysis. J Spinal Disord Tech. 2010; 23(2):89–95. PMID: 20051921.4. Amevo B, Aprill C, Bogduk N. Abnormal instantaneous axes of rotation in patients with neck pain. Spine (Phila Pa 1976). 1992; 17(7):748–756. PMID: 1502637.
Article5. Amevo B, Worth D, Bogduk N. Instantaneous axes of rotation of the typical cervical motion segments: a study in normal volunteers. Clin Biomech (Bristol, Avon). 1991; 6(2):111–117.
Article6. Coric D, Nunley PD, Guyer RD, et al. Prospective, randomized, multicenter study of cervical arthroplasty: 269 patients from the Kineflex|C artificial disc investigational device exemption study with a minimum 2-year follow-up: clinical article. J Neurosurg Spine. 2011; 15(4):348–358. PMID: 21699471.7. Murrey D, Janssen M, Delamarter R, et al. Results of the prospective, randomized, controlled multicenter Food and Drug Administration investigational device exemption study of the ProDisc-C total disc replacement versus anterior discectomy and fusion for the treatment of 1-level symptomatic cervical disc disease. Spine J. 2009; 9(4):275–286. PMID: 18774751.
Article8. Barrey C, Champain S, Campana S, Ramadan A, Perrin G, Skalli W. Sagittal alignment and kinematics at instrumented and adjacent levels after total disc replacement in the cervical spine. Eur Spine J. 2012; 21(8):1648–1659. PMID: 22331142.
Article9. Bible JE, Biswas D, Miller CP, Whang PG, Grauer JN. Normal functional range of motion of the cervical spine during 15 activities of daily living. J Spinal Disord Tech. 2010; 23(1):15–21. PMID: 20051924.
Article10. Bogduk N, Amevo B, Pearcy M. A biological basis for instantaneous centres of rotation of the vertebral column. Proc Inst Mech Eng H. 1995; 209(3):177–183. PMID: 8519407.
Article11. Frobin W, Leivseth G, Biggemann M, Brinckmann P. Sagittal plane segmental motion of the cervical spine: a new precision measurement protocol and normal motion data of healthy adults. Clin Biomech (Bristol, Avon). 2002; 17(1):21–31.
Article12. Wu SK, Kuo LC, Lan HC, Tsai SW, Chen CL, Su FC. The quantitative measurements of the intervertebral angulation and translation during cervical flexion and extension. Eur Spine J. 2007; 16(9):1435–1444. PMID: 17464516.
Article13. Ishii T, Mukai Y, Hosono N, et al. Kinematics of the subaxial cervical spine in rotation in vivo three-dimensional analysis. Spine (Phila Pa 1976). 2004; 29(24):2826–2831. PMID: 15599286.
Article14. Anderst WJ, Lee JY, Donaldson WF 3rd, Kang JD. Six-degrees-of-freedom cervical spine range of motion during dynamic flexion-extension after single-level anterior arthrodesis: comparison with asymptomatic control subjects. J Bone Joint Surg Am. 2013; 95(6):497–506. PMID: 23515984.15. Baillargeon E, Anderst WJ. Sensitivity, reliability and accuracy of the instant center of rotation calculation in the cervical spine during in vivo dynamic flexion-extension. J Biomech. 2013; 46(4):670–676. PMID: 23317757.
Article16. Anderst W, Baillargeon E, Donaldson W, Lee J, Kang J. Motion path of the instant center of rotation in the cervical spine during in vivo dynamic flexion-extension: implications for artificial disc design and evaluation of motion quality after arthrodesis. Spine (Phila Pa 1976). 2013; 38(10):E594–E601. PMID: 23429677.17. Anderst WJ, Baillargeon E, Donaldson WF 3rd, Lee JY, Kang JD. Validation of a noninvasive technique to precisely measure in vivo three-dimensional cervical spine movement. Spine (Phila Pa 1976). 2011; 36(6):E393–E400. PMID: 21372650.
Article18. Wu G, Siegler S, Allard P, et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion--part I: ankle, hip, and spine. International Society of Biomechanics. J Biomech. 2002; 35(4):543–548. PMID: 11934426.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Efficacy of Dynamic Radiographs in Routine Evaluations for Degenerative Cervical Spine Disease
- Analysis of Biomechanical Properties of Whole Cervical Spine under Static Loading with 3-D Finite Element Model
- Delayed or Missed Diagnosis of Cervical Instability after Traumatic Injury: Usefulness of Dynamic Flexion and Extension Radiographs
- Functional Outcomes of Subaxial Spine Injuries Managed With 2-Level Anterior Cervical Corpectomy and Fusion: A Prospective Study
- A Biomechanical Comparison among Three Surgical Methods in Bilateral Subaxial Cervical Facet Dislocation
