Eye Globe Abnormalities on MR and CT in Adults: An Anatomical Approach
- Affiliations
-
- 1Department of Diagnostic Imaging, National University Health System, Singapore 119074. jim.hallinan@gmail.com
- 2National Healthcare Group Eye Institute, Tan Tock Seng Hospital, Level 1, TTSH Medical Centre, Singapore 308433.
- 3Yong Loo Lin School of Medicine, National University of Singapore, Singapore 117597.
- 4Dr. Goh Eye Neuro-Ophthalmic and Low Vision Specialist, Mount Elizabeth Novena Specialist Centre, Singapore 329563.
- 5Department of Neuroradiology, National Neuroscience Institute, Singapore 308433.
- KMID: 2458058
- DOI: http://doi.org/10.3348/kjr.2016.17.5.664
Abstract
- Eye globe abnormalities can be readily detected on dedicated and non-dedicated CT and MR studies. A primary understanding of the globe anatomy is key to characterising both traumatic and non-traumatic globe abnormalities. The globe consists of three primary layers: the sclera (outer), uvea (middle), and retina (inner layer). The various pathological processes involving these layers are highlighted using case examples with fundoscopic correlation where appropriate. In the emergent setting, trauma can result in hemorrhage, retinal/choroidal detachment and globe rupture. Neoplasms and inflammatory/infective processes predominantly occur in the vascular middle layer. The radiologist has an important role in primary diagnosis contributing to appropriate ophthalmology referral, thereby preventing devastating consequences such as vision loss.
MeSH Terms
Figure
-
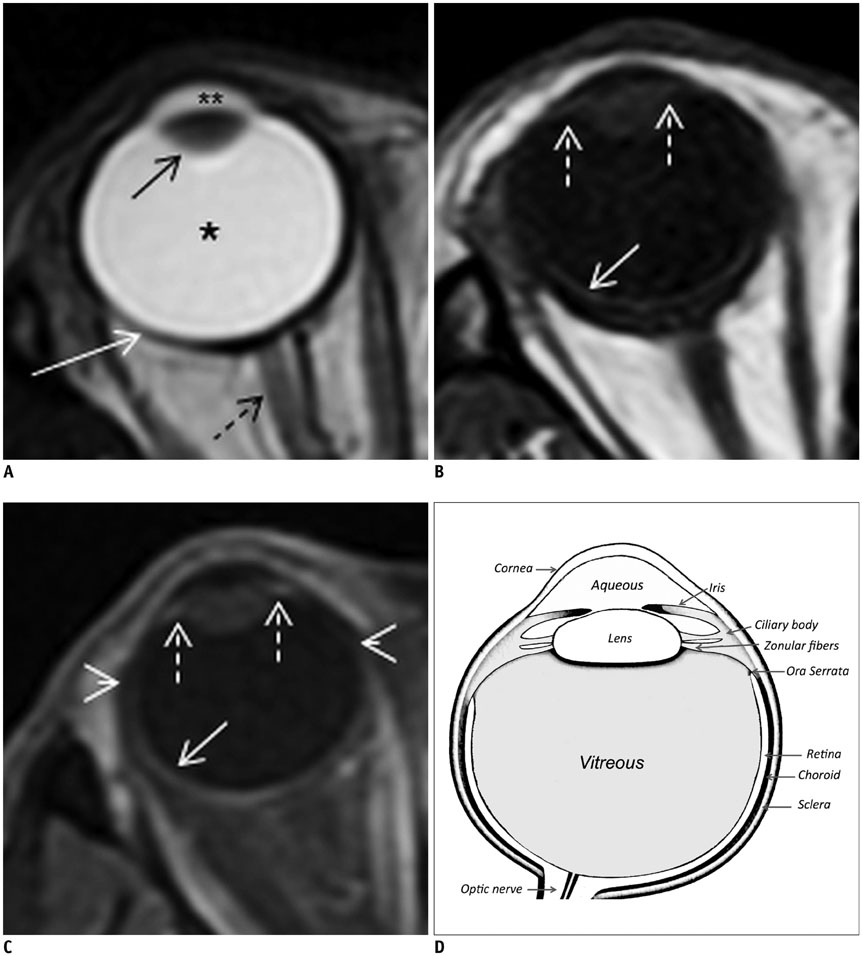
Fig. 1 Normal globe anatomy on orbital MRI. Lens (black arrow) and sclera (white arrow) show hypointense signal on all sequences. A. On axial T2W images, vitreous (*) and aqueous humour in anterior chamber (**) are diffusely hyperintense. Optic nerve is labeled (dashed black arrow). B. Axial T1W image of right globe. Retina and choroid appear as single hyperintense layer (white arrow) with enhancement on fat-saturated post contrast T1W image (C, white arrow). Ciliary bodies form part of choroid (dashed white arrows, B, C). Approximate position of ora serrata is shown (small white arrowheads). D. Anotated illustration of globe for comparison with MRI anatomy. T1W = T1-weighted, T2W = T2-weighted
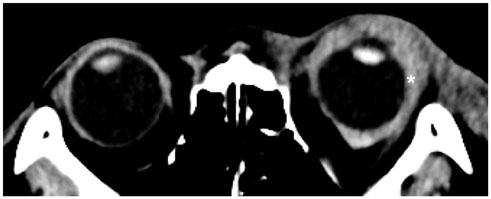
Fig. 2 Axial non-contrast image from post traumatic brain CT scan demonstrates expansion of left episcleral space by hyperdense hematoma (white asterisk), which extends posteriorly to surround globe likely within intra-conal space. Globe appears intact.

Fig. 3 Axial non-contrast enhanced image from orbital CT study on patient with history of Wegener's granulomatosis with posterior scleritis. Bilateral episcleral fluid collections (white asterisks) with distortion of globes are likely due to scleral degeneration or necrosis.
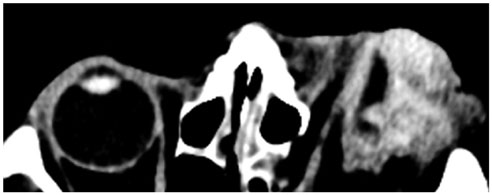
Fig. 4 Axial non-contrast image from brain CT for assessment of direct globe injury shows left globe rupture with complete loss of normal scleral contour, vitreous hemorrhage and surrounding periorbital and episcleral hematomas.
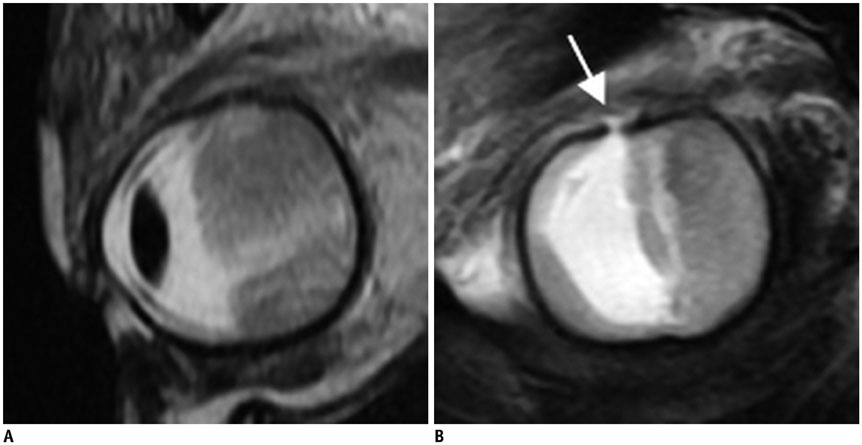
Fig. 5 Sagittal T2W images (A, B) from orbital MRI study to detect post-traumatic globe rupture. Buckling and defect in superior sclera (B, white arrow) with loss of globe volume is consistent with globe rupture. Hypointense material in vitreous is suggestive of hemorrhage. T2W = T2-weighted

Fig. 6 Axial non-contrast image from orbital CT study for assessment of homonymous hemianopia. Bilateral focal protrusions through thinned sclera posteriorly are consistent with posterior staphylomas (white arrows).

Fig. 7 Axial non-contrast image from brain CT assessment of altered mental state shows right phthisis bulbi with irregular, scarred, shrunken right globe and dense internal calcification.
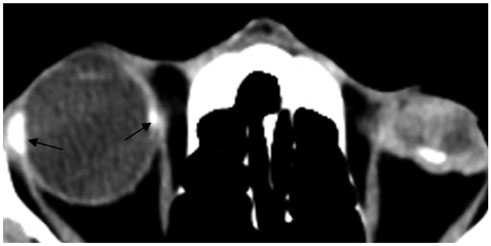
Fig. 8 Axial non-contrast image from brain CT assessment of traumatic head injury shows left phthisis bulbi with irregular, scarred, shrunken globe and left optic disc calcification. Scleral band for treatment of retinal detachment is seen on right (black arrows).
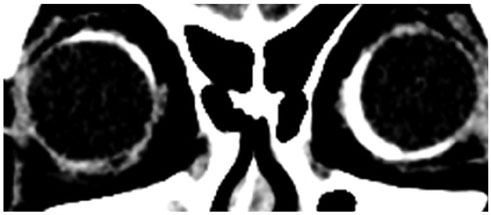
Fig. 9 Coronal non-contrast image from brain CT assessment of frequent falls. Bilateral bands of hyperdensity that do not conform to insertions of extra-ocular muscles, are consistent with prior bilateral scleral bands for treatment of retinal detachment. However, characteristic concavity at site of banding is not seen in this case.

Fig. 10 Axial non-contrast image from brain CT assessment of altered mental state shows bilateral lens prostheses with incidental scleral calcifications at insertion of medial rectus on right and both medial and lateral recti on left. These calcifications represent normal part of aging. Scleral bands would appear more linear, as compared to punctate calcifications observed.

Fig. 11 Axial T2W image from orbital MRI study following direct left globe trauma shows iso- to hypointense episcleral material surrounding globe, consistent with hematoma. Choroidal (black arrow) and retinal (dashed black arrow) detachment is seen in left globe with underlying subchoroidal and subretinal fluid, respectively. T2W = T2-weighted
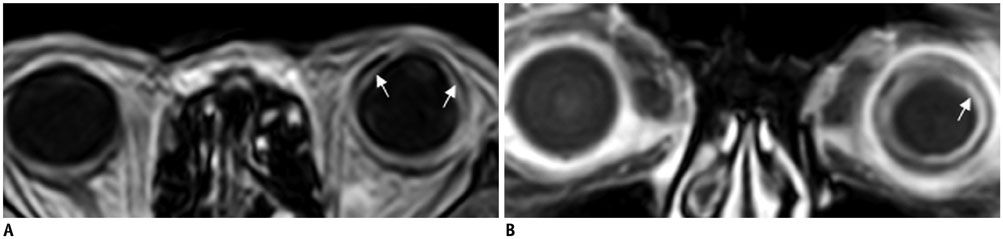
Fig. 12 Axial T1W (A) and coronal T1W post gadolinium (B) images from orbital MRI study for suspected chorioretinal detachment and evaluation for any underlying lesion. Ciliochoroidal detachment extends anterior to expected location of ora serrata (A, white arrows). Enhancement of choroid is noted (B, white arrow), which is expected in detachment due to inflammatory response. Enhancing lesion suggestive of neoplastic cause is absent. T1W = T1-weighted
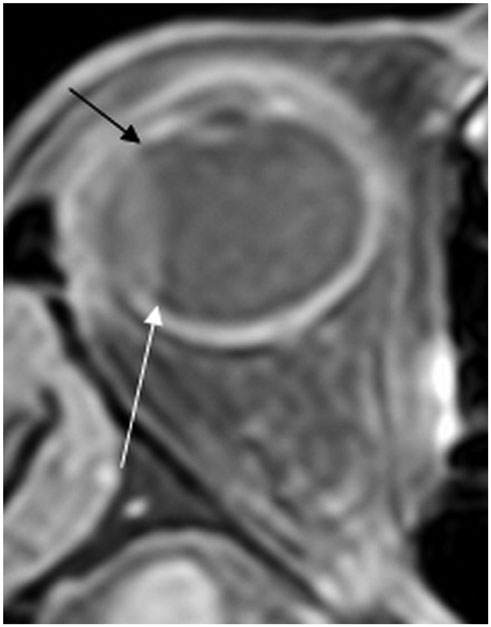
Fig. 13 Axial T1W post gadolinium image from orbital MRI study for right sided visual loss. Right choroidal detachment is seen limited posteriorly at expected location of vortex vein insertion (white arrow) and extending anterior to ora serrata (black arrow). Enhancement of detached choroid is also apparent as in Figure 12. Likewise, enhancing lesion suggestive of neoplastic cause is absent. T1W = T1-weighted
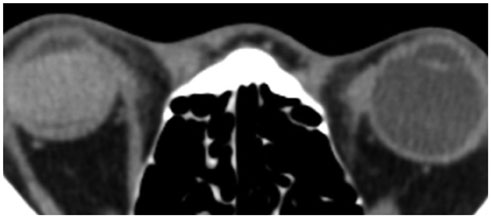
Fig. 14 Axial non-contrast image from brain CT assessment of altered mental state shows hyperdense material filling vitreous cavity on right with no evidence of overlying trauma or periorbital hematoma. This patient had undergone silicone oil injection for treatment of retinal detachment.
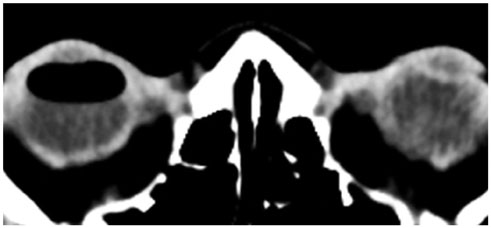
Fig. 15 Axial non-contrast image from brain CT assessment of altered mental state. Gas is noted in anterior vitreous compartment consistent with pneumatic retinopexy typically used in treatment of superior rhegmatogenous retinal detachments. No history of trauma was noted.

Fig. 16 Dedicated orbital MRI study for gradual left visual loss. A. Axial T1WI shows lobulated hyperintense lesion arising in anteromedial left globe with endophytic extension into vitreous. B. T1WI post gadolinium shows enhancement of lesion with considerations including melanoma or hemorrhagic/mucinous metastasis. C. Corresponding photograph shows pigmented lesion arising from inferomedial globe wall with surrounding hemorrhage. Histology was consistent with uveal melanoma. T1W1 = T1-weighted image
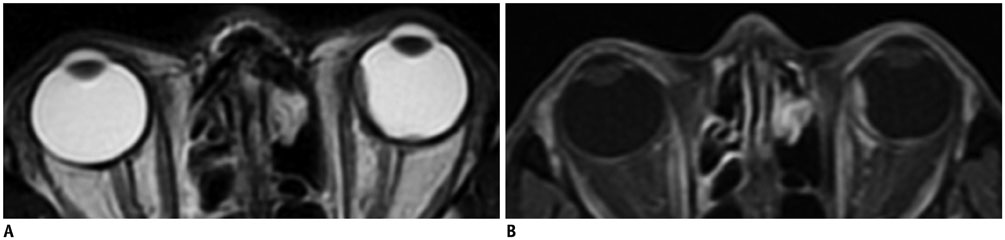
Fig. 17 Male primary lung adenocarcinoma patient presenting with left sided blindness. Axial T2W (A) and axial T1W (B) post gadolinium images from orbital MRI study show T2W hypointense intraocular lesions arising adjacent to sclera in left medial globe and close to left optic nerve head. Medial lesion shows contrast enhancement. Considerations include metastases (highly likely given clinical history) with amelanocytic melanoma (no T1W hypointensity; images not shown), less likely differential. No choroidal detachment is detected. T1W = T1-weighted, T2W = T2-weighted

Fig. 18 Axial T1W post gadolinium images of posterior fossa (A) and orbits (B) from brain and orbital MRI on patient who presented with headaches. Enhancing lesion is observed in region of fourth ventricle complicated by hydrocephalus (not shown). Additional avidly enhancing lesion is seen arising from lateral choroid of left globe without associated chorioretinal detachment. These findings are suggestive of cerebellar and retinal/choroidal hemangioblastomas, although associated cystic component for cerebellar lesion is more typical. Underlying Von Hippel-Lindau disease was key consideration. Metastases are less likely given patient's young age (< 40 years old) and no known history of primary malignancy. Histology following resection of cerebellar lesion confirmed diagnosis of hemangioblastoma. T1W = T1-weighted
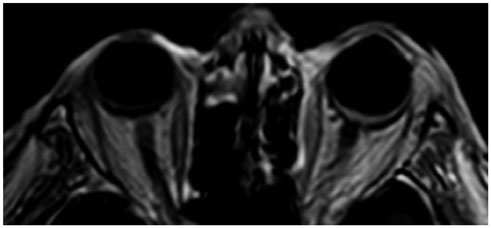
Fig. 19 Axial T1WI post gadolinium image from orbital MRI study performed for globe pain and acute visual loss. Thickening and enhancement of left retina, posterior choroid and optic disc are observed, suggestive of posterior uveitis, which may be associated with inflammatory conditions such as sarcoidosis or infections such as toxoplasma or cytomegalovirus. Underlying neoplasm, e.g., metastasis was less likely as no focal lesion was detected. Patient was not available for follow-up. T1W1 = T1-weighted image
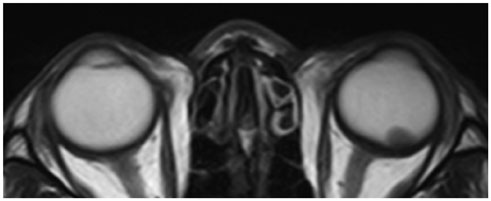
Fig. 20 Axial T2W image from orbital MRI study for evaluation of left visual loss shows left sided lens dislocation (lens luxation) with hypointense lens lying dependently adjacent to retina in posterior vitreous humour. No history of trauma or prior ocular inflammation was noted. Right-sided lens prosthesis is noted. T2W = T2-weighted
Reference
-
1. Roy AA, Davagnanam I, Evanson J. Abnormalities of the globe. Clin Radiol. 2012; 67:1011–1022.2. Van Tassel P, Mafee MF, Atlas SW, Galetta SL. Chapter 23. Eye, orbit and visual system. In : Atlas SW, editor. Magnetic resonance imaging of the brain and spine. 4th ed. Philadelphia: Lippincott Williams & Wilkins;2009. Volume 2:p. 1258–1363.3. Mafee MF, Karimi A, Shah J, Rapoport M, Ansari SA. Anatomy and pathology of the eye: role of MR imaging and CT. Neuroimaging Clin N Am. 2005; 15:23–47.4. Goh PS, Gi MT, Charlton A, Tan C, Gangadhara Sundar JK, Amrith S. Review of orbital imaging. Eur J Radiol. 2008; 66:387–395.5. Lane JI, Watson RE Jr, Witte RJ, McCannel CA. Retinal detachment: imaging of surgical treatments and complications. Radiographics. 2003; 23:983–994.6. Ahmad SM, Esmaeli B. Metastatic tumors of the orbit and ocular adnexa. Curr Opin Ophthalmol. 2007; 18:405–413.7. Laver NV, McLaughlin ME, Duker JS. Ocular melanoma. Arch Pathol Lab Med. 2010; 134:1778–1784.8. Smoker WR, Gentry LR, Yee NK, Reede DL, Nerad JA. Vascular lesions of the orbit: more than meets the eye. Radiographics. 2008; 28:185–204. quiz 325.9. LeBedis CA, Sakai O. Nontraumatic orbital conditions: diagnosis with CT and MR imaging in the emergent setting. Radiographics. 2008; 28:1741–1753.10. Kubal WS. Imaging of orbital trauma. Radiographics. 2008; 28:1729–1739.11. Rumboldt Z, Moses C, Wieczerzynski U, Saini R. Diffusion-weighted imaging, apparent diffusion coefficients, and fluid-attenuated inversion recovery MR imaging in endophthalmitis. AJNR Am J Neuroradiol. 2005; 26:1869–1872.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Role of Orbital Computed Tomography as a Prognostic Indicator for Open Globe Injury
- A Case of Traumatic Globe Luxation
- Traumatic Displacement of the Globe into the Ethmoid Sinus: Case Report
- Traumatic Displacement of the Globe into the Maxillary Sinus: Case Report
- CT and MR Findings of Persistent Hyperplastic Primary Vitreous(PH PV)
