Minimally Invasive Anterior Decompression Technique without Instrumented Fusion for Huge Ossification of the Posterior Longitudinal Ligament in the Thoracic Spine: Technical Note And Literature Review
- Affiliations
-
- 1Department of Neurosurgery, Spine Health Wooridul Hospital, Busan, Korea. bswooridul@gmail.com
- 2Department of Orthopedics, Tai Shin Hospital, Taichung, Taiwan.
- 3Department of Neurosurgery, Spine Health Wooridul Hospital Gangnam, Seoul, Korea.
- KMID: 2457968
- DOI: http://doi.org/10.3340/jkns.2017.0404.017
Abstract
OBJECTIVE
Several surgical methods have been reported for treatment of ossification of the posterior longitudinal ligament (OPLL) in the thoracic spine. Despite rapid innovation of instruments and techniques for spinal surgery, the postoperative outcomes are not always favorable. This article reports a minimally invasive anterior decompression technique without instrumented fusion, which was modified from the conventional procedure. The authors present 2 cases of huge beak-type OPLL. Patients underwent minimally invasive anterior decompression without fusion. This method created a space on the ventral side of the OPLL without violating global thoracic spinal stability. Via this space, the OPLL and anterior lateral side of the dural sac can be seen and manipulated directly. Then, total removal of the OPLL was accomplished. No orthosis was needed. In this article, we share our key technique and concepts for treatment of huge thoracic OPLL.
METHODS
Case 1. 51-year-old female was referred to our hospital with right lower limb radiating pain and paresis. Thoracic OPLL at T6-7 had been identified at our hospital, and conservative treatment had been tried without success. Case 2. This 54-year-old female with a 6-month history of progressive gait disturbance and bilateral lower extremity radiating pain (right>left) was admitted to our institute. She also had hypoesthesia in both lower legs. Her symptoms had been gradually progressing. Computed tomography scans showed massive OPLL at the T9-10 level. Magnetic resonance imaging of the thoracolumbar spine demonstrated ventral bony masses with severe anterior compression of the spinal cord at the same level.
RESULTS
We used this surgical method in 2 patients with a huge beaked-type OPLL in the thoracic level. Complete removal of the OPLL via anterior decompression without instrumented fusion was accomplished. The 1st case had no intraoperative or postoperative complications, and the 2nd case had 1 intraoperative complication (dural tear) and no postoperative complications. There were no residual symptoms of the lower extremities.
CONCLUSION
This surgical technique allows the surgeon to safely and effectively perform minimally invasive anterior decompression without instrumented fusion via a transthoracic approach for thoracic OPLL. It can be applied at the mid and lower level of the thoracic spine and could become a standard procedure for treatment of huge beak-type thoracic OPLL.
Keyword
MeSH Terms
Figure
-
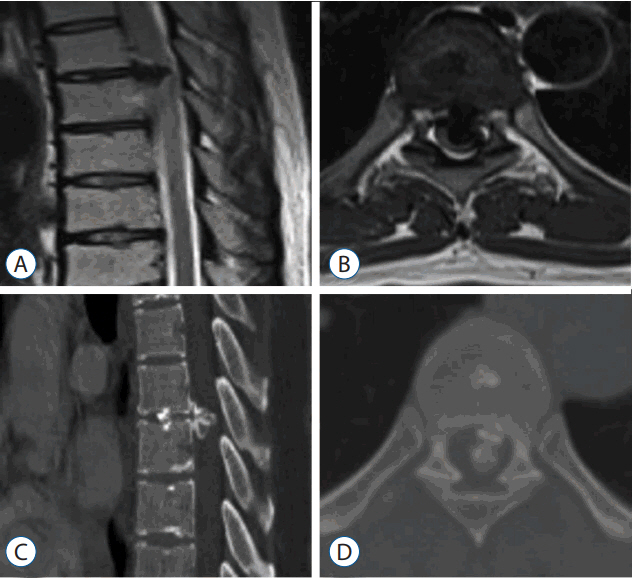
Fig. 1 Preoperative sagittal and axial magnetic resonance (A and B) and computed tomography (C and D) images showing a huge beak-type ossification of the posterior longitudinal ligament at the T6–7 level with severe compression of the spinal cord.
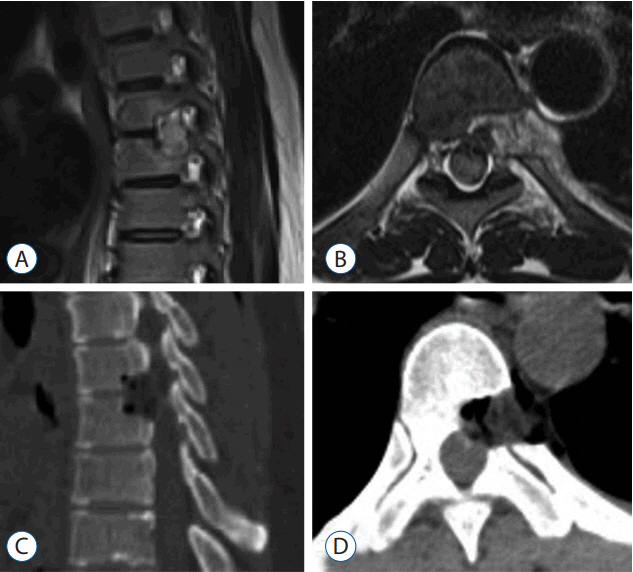
Fig. 2 Postoperative sagittal (A) and axial (B) magnetic resonance and sagittal (C) and axial (D) computed tomography images reveal complete removal of the ossified posterior longitudinal ligament and total decompression of the spinal cord at the T6–7 level.
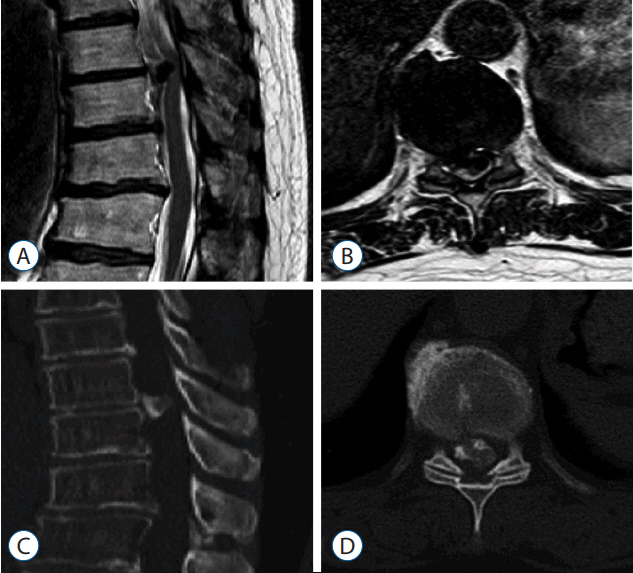
Fig. 3 Preoperative thoracolumbar magnetic resonance (A and B) and computed tomography (C and D) images show the beak-type ossification of the posterior longitudinal ligament at T9–10, which had compressed the spinal cord.
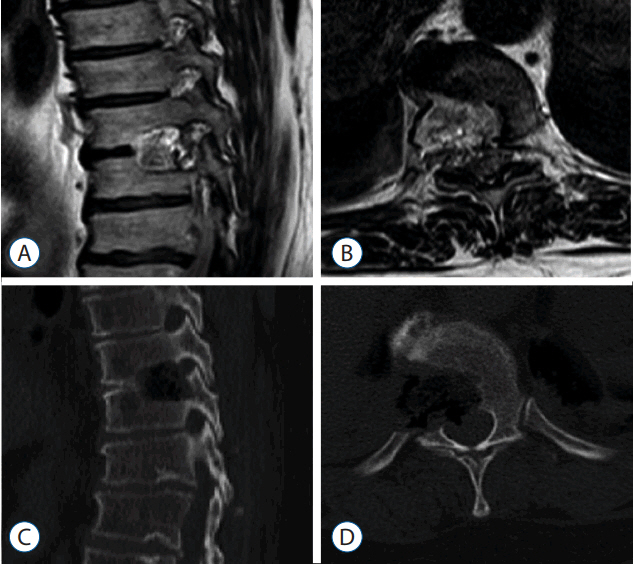
Fig. 4 Postoperative sagittal (A) and axial (B) magnetic resonance and sagittal (C) and axial (D) computed tomography images show complete removal of the ossified posterior longitudinal ligament and total decompression of the spinal cord at the T9–10 level.

Fig. 5 A: The endothoracic fascia opening can be followed posteriorly to the proximal rib head, which was excised. B: The rostral portion of the pedicle directly caudal to the disc space can also be drilled down to improve exposure of the dural sac and ossification of the posterior longitudinal ligament.

Fig. 6 A: After releasing the adhesion between the ossification of the posterior longitudinal ligament (OPLL) and the dural sac by dissection, the OPLL was removed. B: Bleeding was controlled using Avitene and cottonoids.
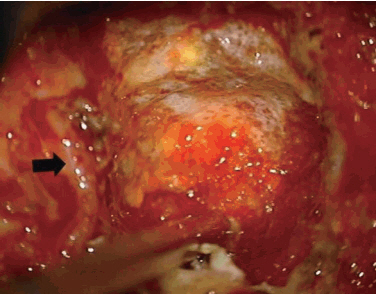
Fig. 7 During operation, the segmental artery (black arrow) was preserved.
Reference
-
References
1. Abumi K, Suda K. Surgical strategy for thoracic OPLL. Orthop Surg Traumatol. 45:615–621. 2002.2. Aizawa T, Sato T, Sasaki H, Matsumoto F, Morozumi N, Kusakabe T, et al. Results of surgical treatment for thoracic myelopathy: minimum 2-year follow-up study in 132 patients. J Neurosurg Spine. 7:13–20. 2007.
Article3. Fujimura Y, Nishi Y, Nakamura M, Toyama Y, Suzuki N. Long-term follow-up study of anterior decompression and fusion for thoracic myelopathy resulting from ossification of the posterior longitudinal ligament. Spine (Phila Pa 1976). 22:305–311. 1997.
Article4. Fujimura Y, Nishi Y, Nakamura M, Watanabe M, Matsumoto M. Myelopathy secondary to ossification of the posterior longitudinal ligament of the thoracic spine treated by anterior decompression and bony fusion. Spinal Cord. 35:777–784. 1997.
Article5. Ido K, Shimizu K, Nakayama Y, Yamamuro T, Shikata J, Matsushita M, et al. Anterior decompression and fusion for ossification of posterior longitudinal ligament in the thoracic spine. J Spinal Disord. 8:317–323. 1995.
Article6. Kato S, Kawahara N, Tomita K, Murakami H, Demura S, Fujimaki Y. Effects on spinal cord blood flow and neurologic function secondary to interruption of bilateral segmental arteries which supply the artery of Adamkiewicz: an experimental study using a dog model. Spine (Phila Pa 1976). 33:1533–1541. 2008.
Article7. Kawahara N, Tomita K, Murakami H, Hato T, Demura S, Sekino Y, et al. Circumspinal decompression with dekyphosis stabilization for thoracic myelopathy due to ossification of the posterior longitudinal ligament. Spine (Phila Pa 1976). 33:39–46. 2008.
Article8. Kawakami N, Mimatsu K, Kato F, Sato K, Matsuyama Y. Intraoperative ultrasonographic evaluation of the spinal cord in cervical myelopathy. Spine (Phila Pa 1976). 19:34–41. 1994.
Article9. Kojima T, Waga S, Kubo Y, Matsubara T. Surgical treatment of ossification of the posterior longitudinal ligament in the thoracic spine. Neurosurgery. 34:854–858. discussion 858. 1994.
Article10. Kurosa Y, Yamaura I, Nakai O, Shinomiya K. Selecting a surgical method for thoracic myelopathy caused by ossification of the posterior longitudinal ligament. Spine (Phila Pa 1976). 21:1458–1466. 1996.
Article11. Lazorthes G, Gouaze A, Zadeh JO, Santini JJ, Lazorthes Y, Burdin P. Arterial vascularization of the spinal cord. Recent studies of the anastomotic substitution pathways. J Neurosurg. 35:253–262. 1971.12. Matsumoto M, Chiba K, Toyama Y, Takeshita K, Seichi A, Nakamura K, et al. Surgical results and related factors for ossification of posterior longitudinal ligament of the thoracic spine: a multi-institutional retrospective study. Spine (Phila Pa 1976). 33:1034–1041. 2008.
Article13. Matsuyama Y, Sakai Y, Katayama Y, Imagama S, Ito Z, Wakao N, et al. Indirect posterior decompression with corrective fusion for ossification of the posterior longitudinal ligament of the thoracic spine: is it possible to predict the surgical results? Eur Spine J. 18:943–948. 2009.
Article14. Matsuyama Y, Yoshihara H, Tsuji T, Sakai Y, Yukawa Y, Nakamura H, et al. Surgical outcome of ossification of the posterior longitudinal ligament (OPLL) of the thoracic spine: implication of the type of ossification and surgical options. J Spinal Disord Tech. 18:492–498. discussion 498. 2005.15. Min JH, Jang JS, Lee SH. Clinical results of ossification of the posterior longitudinal ligament (OPLL) of the thoracic spine treated by anterior decompression. J Spinal Disord Tech. 21:116–119. 2008.
Article16. Murakami H, Kawahara N, Tomita K, Demura S, Kato S, Yoshioka K. Does interruption of the artery of Adamkiewicz during total en bloc spondylectomy affect neurologic function? Spine (Phila Pa 1976). 35:E1187–E1192. 2010.
Article17. Ohtsuka K, Terayama K, Tsuchiya T, Wada K, Furukawa K, Ohkubo M. A surgical procedure of the anterior decompression of the thoracic spinal cord through the posterior approach. Orthop Surg Traumatol. 26:1083–1090. 1983.18. Takahata M, Ito M, Abumi K, Kotani Y, Sudo H, Minami A. Clinical results and complications of circumferential spinal cord decompression through a single posterior approach for thoracic myelopathy caused by ossification of posterior longitudinal ligament. Spine (Phila Pa 1976). 33:1199–1208. 2008.
Article19. Tomita K, Kawahara N, Baba H, Kikuchi Y, Nishimura H. Circumspinal decompression for thoracic myelopathy due to combined ossification of the posterior longitudinal ligament and ligamentum flavum. Spine (Phila Pa 1976). 15:1114–1120. 1990.
Article20. Tokuhashi Y, Matsuzaki H, Oda H, Uei H. Effectiveness of posterior decompression for patients with ossification of the posterior longitudinal ligament in the thoracic spine: usefulness of the ossification-kyphosis angle on MRI. Spine (Phila Pa 1976). 31:E26–E30. 2006.21. Tsuyama N. Ossification of the posterior longitudinal ligament of the spine. Clin Orthop Relat Res. 184:71–84. 1984.
Article22. Tsuzuki N, Hirabayashi S, Abe R, Saiki K. Staged spinal cord decompression through posterior approach for thoracic myelopathy caused by ossification of posterior longitudinal ligament. Spine (Phila Pa 1976). 26:1623–1630. 2001.
Article23. Yamazaki M, Mochizuki M, Ikeda Y, Sodeyama T, Okawa A, Koda M, et al. Clinical results of surgery for thoracic myelopathy caused by ossification of the posterior longitudinal ligament: operative indication of posterior decompression with instrumented fusion. Spine (Phila Pa 1976). 31:1452–1460. 2006.
Article24. Yonenobu K, Korkusuz F, Hosono N, Ebara S, Ono K. Lateral rhachotomy for thoracic spinal lesions. Spine (Phila Pa 1976). 15:1121–1125. 1990.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Retraction: Minimally Invasive Anterior Decompression Technique without Instrumented Fusion for Huge Ossification of the Posterior Longitudinal Ligament in the Thoracic Spine: Technical Note And Literature Review
- Treatment of Ossification of Posterior Longitudinal Ligament in Cervical Spine with Anterior Fusion and Anterior Decompression: Report of 3 Cases
- Anterior Decompression and Interbody Fusion for Ossification of the Posterior Longitudinal Ligament of the Cervical Spine: Case Report
- Ossification of the Posterior Longitudinal Ligament: 2 cases report
- Circumferential Spinal Cord Decompression through a Single Posterior Approach with Microendoscopy for Thoracic and Thoracolumbar Ossification of the Posterior Longitudinal Ligament
