Pediatr Gastroenterol Hepatol Nutr.
2019 Sep;22(5):487-492. 10.5223/pghn.2019.22.5.487.
Waardenburg Syndrome Type IV De Novo SOX10 Variant Causing Chronic Intestinal Pseudo-Obstruction
- Affiliations
-
- 1Division of Pediatric Surgery, Department of Surgery, University of Miami Miller School of Medicine, Miami, FL, United States. ahogan@med.miami.edu
- 2Division of Clinical and Translational Genetics, Department of Human Genetics, University of Miami Miller School of Medicine, Miami, FL, United States.
- KMID: 2457751
- DOI: http://doi.org/10.5223/pghn.2019.22.5.487
Abstract
- Waardenburg syndrome (WS) type IV is characterized by pigmentary abnormalities, deafness and Hirschsprung's disease. This syndrome can be triggered by dysregulation of the SOX10 gene, which belongs to the SOX (SRY-related high-mobility group-box) family of genes. We discuss the first known case of a SOX10 frameshift mutation variant defined as c.895delC causing WS type IV without Hirschsprung's disease. This female patient of unrelated Kuwaiti parents, who tested negative for cystic fibrosis and Hirschsprung's disease, was born with meconium ileus and malrotation and had multiple surgical complications likely due to chronic intestinal pseudo-obstruction. These complications included small intestinal necrosis requiring resection, development of a spontaneous fistula between the duodenum and jejunum after being left in discontinuity, and short gut syndrome. This case and previously reported cases demonstrate that SOX10 gene sequencing is a consideration in WS patients without aganglionosis but with intestinal dysfunction.
Keyword
MeSH Terms
Figure
-
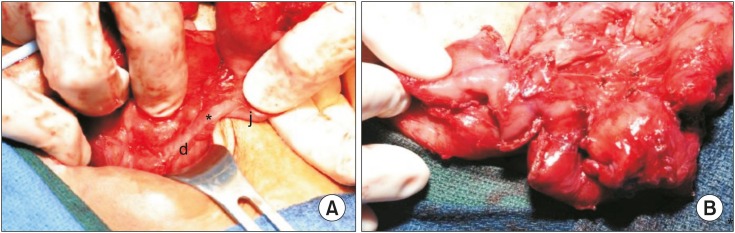
Fig. 1 (A) Intraoperative view of the entero-enteric fistula (asterisk) from the second portion of duodenum (d) to the proximal end of the former closed loop mid-jejunal segment (j). (B) View of the completed serial transverse enteroplasty.
Reference
-
1. Jalilian N, Tabatabaiefar MA, Alimadadi H, Noori-Daloii MR. SOX10 mutation causes Waardenburg syndrome associated with distinctive phenotypic features in an Iranian family: a clue for phenotype-directed genetic analysis. Int J Pediatr Otorhinolaryngol. 2017; 96:122–126. PMID: 28390600.
Article2. Bondurand N, Dastot-Le Moal F, Stanchina L, Collot N, Baral V, Marlin S, et al. Deletions at the SOX10 gene locus cause Waardenburg syndrome types 2 and 4. Am J Hum Genet. 2007; 81:1169–1185. PMID: 17999358.
Article3. Waardenburg PJ. A new syndrome combining developmental anomalies of the eyelids, eyebrows and nose root with pigmentary defects of the iris and head hair and with congenital deafness. Am J Hum Genet. 1951; 3:195–253. PMID: 14902764.4. Pingault V, Girard M, Bondurand N, Dorkins H, Van Maldergem L, Mowat D, et al. SOX10 mutations in chronic intestinal pseudo-obstruction suggest a complex physiopathological mechanism. Hum Genet. 2002; 111:198–206. PMID: 12189494.
Article5. Chaoui A, Watanabe Y, Touraine R, Baral V, Goossens M, Pingault V, et al. Identification and functional analysis of SOX10 missense mutations in different subtypes of Waardenburg syndrome. Hum Mutat. 2011; 32:1436–1449. PMID: 21898658.6. Wilcox DT, Borowitz DS, Stovroff MC, Glick PL. Chronic intestinal pseudo-obstruction with meconium ileus at onset. J Pediatr. 1993; 123:751–752. PMID: 8229485.
Article7. Pini Prato A, Rossi V, Fiore M, Avanzini S, Mattioli G, Sanfilippo F, et al. Megacystis, megacolon, and malrotation: a new syndromic association? Am J Med Genet A. 2011; 155A:1798–1802. PMID: 21739599.
Article8. Devane SP, Coombes R, Smith VV, Bisset WM, Booth IW, Lake BD, et al. Persistent gastrointestinal symptoms after correction of malrotation. Arch Dis Child. 1992; 67:218–221. PMID: 1543383.
Article9. Lehtonen HJ, Sipponen T, Tojkander S, Karikoski R, Järvinen H, Laing NG, et al. Segregation of a missense variant in enteric smooth muscle actin γ-2 with autosomal dominant familial visceral myopathy. Gastroenterology. 2012; 143:1482–1491.e3. PMID: 22960657.
Article10. Milunsky A, Baldwin C, Zhang X, Primack D, Curnow A, Milunsky J. Diagnosis of chronic intestinal pseudo-obstruction and megacystis by sequencing the ACTG2 gene. J Pediatr Gastroenterol Nutr. 2017; 65:384–387. PMID: 28422808.
Article11. Wangler MF, Beaudet AL. ACTG2-related disorders. In : Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K, editors. GeneReviews®. Seattle (WA): University of Washington;1993.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Megacystis Associated with Primary Chronic Intestinal Pseudoobstruction
- A case of chronic intestinal pseudo-obstruction syndrome
- Identification of a Novel De Novo Variant in the PAX3 Gene in Waardenburg Syndrome by Diagnostic Exome Sequencing: The First Molecular Diagnosis in Korea
- Chronic Idiopathic Intestinal Pseudo-obstruction in Adult: A Case Report with a Clinical Analysis of Other Reported Cases in Korean Literature
- Acute Intestinal Pseudo-Obstruction in a Patient with MELAS Syndrome
