Diagnostic Approach to a Soft Tissue Mass
- Affiliations
-
- 1Department of Orthopaedic Surgery, Kyung Hee University Hospital at Gangdong, College of Medicine, Kyung Hee University, Seoul, Korea. mozart13@khu.ac.kr
- KMID: 2455497
- DOI: http://doi.org/10.4055/jkoa.2019.54.4.293
Abstract
- Soft tissue masses of the extremities and torso are a common problem encountered by orthopaedic surgeons. Although these soft tissue masses are often benign, orthopaedic surgeons need to recognize the key features differentiating benign and malignant masses. An understanding of the epidemiology and clinical presentation of soft tissue masses is needed to develop a practical approach for evaluation and surgical management. Size and depth are the two most important factors on which triage decisions should be based. In a differential diagnosis of a tumor, it is important to know the characteristics of the soft tissue mass through detailed history taking and physical examinations before the diagnostic procedures. A variety of imaging studies, such as simple radiography, ultrasound, magnetic resonance imaging, positron emission tomography, computed tomography, bone scan, and angiography can be used to diagnose tumors. Know the ledge of advantages and disadvantages of each imaging study is essential for confirming the characteristics of the tumor that can be observed in the image. In particular, ultrasonography is convenient because it can be performed easily in an outpatient clinic and its cost is lower than other image studies. On the other hand, the accuracy of the test is affected by the skill of the examiner. A biopsy should be performed to confirm the tumor and be performed after all imaging studies have been done but before the final treatment of soft tissue tumors. When a biopsy is to be performed, careful attention to detail with respect to multidisciplinary coordination beforehand, cautious execution of the procedure to minimize complications, and expedient follow-up and referral to a musculoskeletal oncologist when appropriate, are essential.
Keyword
MeSH Terms
Figure
-
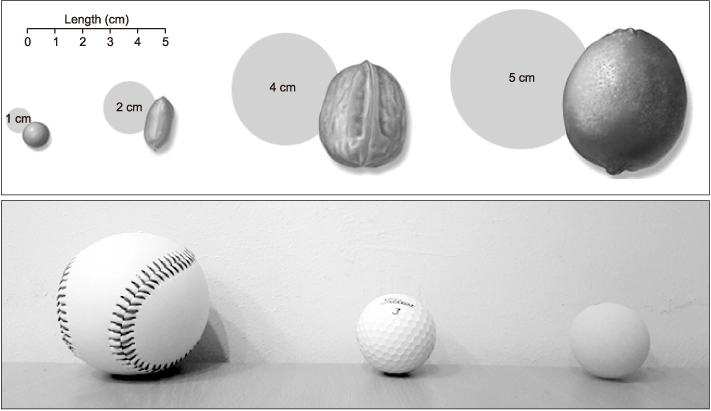
Figure 1 Size description of soft tissue masses (baseball 7.2 cm, golf ball 4.6 cm, table tennis ball 4 cm).
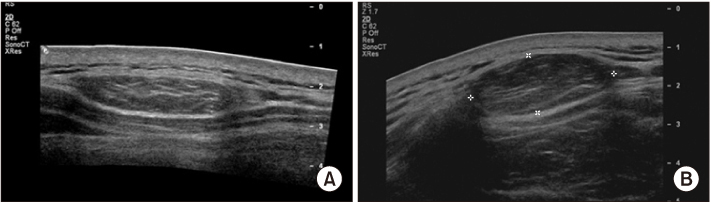
Figure 2 Ultrasonography findings of soft tissue masses. (A) These appearances are characteristic of lipoma. (B) Well differentiated liposarcoma. Ultrasound image shows an encapsulated subcutaneous mass isoechoic to the adjacent subcutaneous fat and fine internal echogenic striations parallel to the long axis of the mass. Lipoma and well differentiated liposarcoma are difficult to differential diagnosis completely by ultrasound.
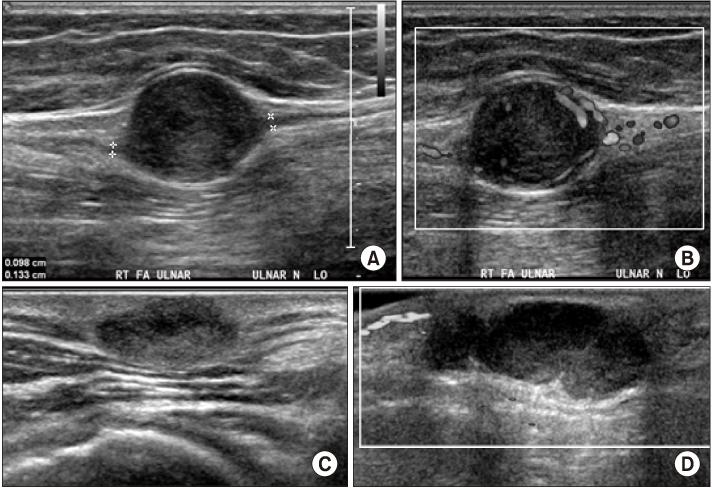
Figure 3 Sonographic images of schwannoma. (A) Longitudinal forearm ultrasound shows a fusiform heterogeneous, hypoechoic mass in continuity with the ulnar nerve with posterior acoustic enhancement. Note the entering and exiting components of the ulnar nerve. (B) Transverse color Doppler ultrasound of the same lesion shows a moderate degree of intralesional hypervascularity. Note the moderate posterior acoustic enhancement. (C) Oval shaped mass with heterogeneous echogenicity with no continuity with the nerve of shoulder lesion. (D) Well-defined, lobulated, low echoic mass ulnar to the 5th distal interphalangeal joint with no increased vascularity.

Figure 4 Magnetic resonance imagings of leiomyosarcoma. Relatively well-defined superficial soft tissue mass in the posterolateral aspect of the right buttock at the greater trochanteric level, (A) T1 weighted image with intermediate signal intensity (higher signal to the muscle), (B) T2 weighted fat suppressed image with bright high signal and intermediate signal intensity, (C) T1 weighted fat suppressed contrast enhancement image with strong enhancement (no enhancement in the bright high signal portion on T1 weighted image.

Figure 5 Magnetic resonance imagings (MRIs) of lipoma (A), liposarcoma (B, pleomorphic). (A-a) Axial T2 weighted image (T2WI) MRI shows a homogeneous, high signal, fatty mass along the medial aspect of the proximal arm. The mass has the same signal intensity as the adjacent subcutaneous fat. No nodules or thick septa can be seen. A blood vessel is present along the deep border of the mass. (A-b) Axial T1 weighted fat suppressed image (T1WI FS MRI) with contrast enhancement shows the signal intensity of the lipoma is entirely suppressed, similar to the subcutaneous fat, to become homogeneously low. The single high signal focus is vascular. (B-a) Axial T1WI MRI shows an irregular and lobulating intramuscular mass in the anterolateral portion of the mid-thigh, heterogeneously, iso to low signal intensity. (B-b) Axial T2WI shows mixed signal intensity. (B-c) T1WI FS MRI shows heterogeneous enhancement. A malignant finding in MRI, pleomorphic liposarcoma in the pathology examination.
Reference
-
1. Springfield D. Evaluation of soft tissue tumors. Instr Course Lect. 1999; 48:617–619.2. Silverstein E, Gibbs CP. Classification and imaging of soft-tissue tumors. In : Schwartz HS, editor. Orthopaedic knowledge update. Musculoskeletal tumors 2. 2nd ed. Rosemont (IL): American Academy of Orthopaedic Surgeons;2007. p. 289–299.3. Frassica FJ, McCarthy EF, Bluemke DA. Soft-tissue masses: when and how to biopsy. Instr Course Lect. 2000; 49:437–442.4. Frassica FJ, Thompson RC Jr. Evaluation, diagnosis, and classification of benign soft-tissue tumors. J Bone joint Surg. 1996; 78:126–140.5. Sim FH, Frassica FJ, Frassica DA. Soft tissue tumors: diagnosis, evaluation, and management. J Am Acad Orthop Surg. 1994; 2:201–211.6. Schuetze SM. Imaging and response in soft tissue sarcomas. Hematol Oncol Clin North Am. 2005; 19:471–487. vi.
Article7. Manaster BJ. Soft-tissue masses: optimal imaging protocol and reporting. AJR Am J Roentgenol. 2013; 201:505–514.
Article8. Jones BC, Fayad LM. Musculoskeletal tumor imaging: focus on emerging techniques. Semin Roentgenol. 2017; 52:269–281.
Article9. Shapeero LG, Vanel D, Verstraete KL, Bloem JL. Fast magnetic resonance imaging with contrast for soft tissue sarcoma viability. Clin Orthop Relat Res. 2002; 397:212–227.
Article10. Vanel D, Bonvalot S, Guinebretière JM, Petrow P, Dromain C, Caillet H. MR imaging in the evaluation of isolated limb perfusion: a prospective study of 18 cases. Skeletal Radiol. 2004; 33:150–156.
Article11. Weiss SW, Goldblum J, Enzinger FM. Enzinger and Weiss's soft tissue tumors. 4th ed. St. Louis (MO): Mosby;2001.12. Peabody TD, Gibbs CP Jr, Simon MA. Evaluation and staging of musculoskeletal neoplasms. J Bone Joint Surg Am. 1998; 80:1204–1208.13. Aoki J, Endo K, Watanabe H, et al. FDG-PET for evaluation musculoskeletal tumors: a review. J Orthop Sci. 2003; 8:435–441.14. Aoki J, Watanabe H, Shinozaki T, et al. FDG-PET for preoperative differential diagnosis between benign and malignant soft tissue masses. Skeletal Radiol. 2003; 32:133–138.
Article15. Aoki J, Watanabe H, Shinozaki T, et al. FDG PET of primary benign and malignant bone tumors: standardized uptake value in 52 lesions. Radiology. 2001; 219:774–777.
Article16. Dimitrakopoulou-Strauss A, Strauss LG, Schwarzbach M, et al. Dynamic PET 18F-FDG studies in patients with primary and recurrent soft-tissue sarcomas: impact on diagnosis and correlation with grading. J Nucl Med. 2001; 42:713–720.17. Satoh K, Sadowski SM, Dieckmann W, et al. 18F-FDG PET/CT volumetric parameters are associated with tumor grade and metastasis in pancreatic neuroendocrine tumors in von hippel-lindau disease. Ann Surg Oncol. 2016; 23:S714–S721.
Article18. Tomimaru Y, Eguchi H, Tatsumi M, et al. Clinical utility of 2-[(18)F] fluoro-2-deoxy-D-glucose positron emission tomography in predicting World Health Organization grade in pancreatic neuroendocrine tumors. Surgery. 2015; 157:269–276.
Article19. Vernon CB, Eary JF, Rubin BP, Conrad EU 3rd, Schuetze S. FDG PET imaging guided re-evaluation of histopathologic response in a patient with high-grade sarcoma. Skeletal Radiol. 2003; 32:139–142.
Article20. Mankin HJ, Lange TA, Spanier SS. The hazards of biopsy in patients with malignant primary bone and soft tissue tumors. J Bone Joint Surg Am. 1982; 64:1121–1127.21. Mankin HJ, Hornicek FJ. Diagnosis, classification, and management of soft tissue sarcomas. Cancer Control. 2005; 12:5–21.
Article22. Canter RJ. Surgical approach for soft tissue sarcoma: standard of care and future approaches. Curr Opin Oncol. 2015; 27:343–348.
