The effects of hard and soft tissue grafting and individualization of healing abutments at immediate implants: an experimental study in dogs
- Affiliations
-
- 1Clinic of Fixed and Removable Prosthodontics and Dental Material Science, University of Zurich, Zürich, Switzerland.
- 2Department of Periodontology, Research Institute for Periodontal Regeneration, Yonsei University College of Dentistry, Seoul, Korea. DRJEW@yuhs.ac
- 3Department of Periodontology, Julius-Maximilians-University of Würzburg, Würzburg, Germany.
- KMID: 2454087
- DOI: http://doi.org/10.5051/jpis.2019.49.3.171
Abstract
- PURPOSE
To evaluate the effects of intra-alveolar socket grafting, subepithelial connective tissue grafts, and individualized abutments on peri-implant hard and soft tissue outcomes following immediate implant placement.
METHODS
This randomized experimental study employed 5 mongrel dogs, with 4 sites per dog (total of 20 sites). The mesial roots of P3 and P4 were extracted in each hemimandible and immediate dental implants were placed. Each site was randomly assigned to 1 of 4 different treatment groups: standardized healing abutment (control group), alloplastic bone substitute material (BSS) + standardized healing abutment (SA group), BSS + individualized healing abutment (IA group), and BSS + individualized healing abutment + a subepithelial connective tissue graft (IAG group). Clinical, histological, and profilometric analyses were performed. The intergroup differences were calculated using the Bonferroni test, setting statistical significance at P<0.05.
RESULTS
Clinically, the control and SA groups demonstrated a coronal shift in the buccal height of the mucosa (0.88±0.48 mm and 0.37±1.1 mm, respectively). The IA and IAG groups exhibited an apical shift of the mucosa (−0.7±1.15 mm and −1.1±0.96 mm, respectively). Histologically, the SA and control groups demonstrated marginal mucosa heights of 4.1±0.28 mm and 4.0±0.53 mm relative to the implant shoulder, respectively. The IA and IAG groups, in contrast, only showed a height of 2.6 mm. In addition, the height of the mucosa in relation to the most coronal buccal bone crest or bone substitute particles was not significantly different among the groups. Volumetrically, the IA group (−0.73±0.46 mm) lost less volume on the buccal side than the control (−0.93±0.44 mm), SA (−0.97±0.73 mm), and IAG (−0.88±0.45 mm) groups.
CONCLUSIONS
The control group demonstrated the most favorable change of height of the margo mucosae and the largest dimensions of the peri-implant soft tissues. However, the addition of a bone substitute material and an individualized healing abutment resulted in slightly better preservation of the peri-implant soft tissue contour.
Keyword
MeSH Terms
Figure
-
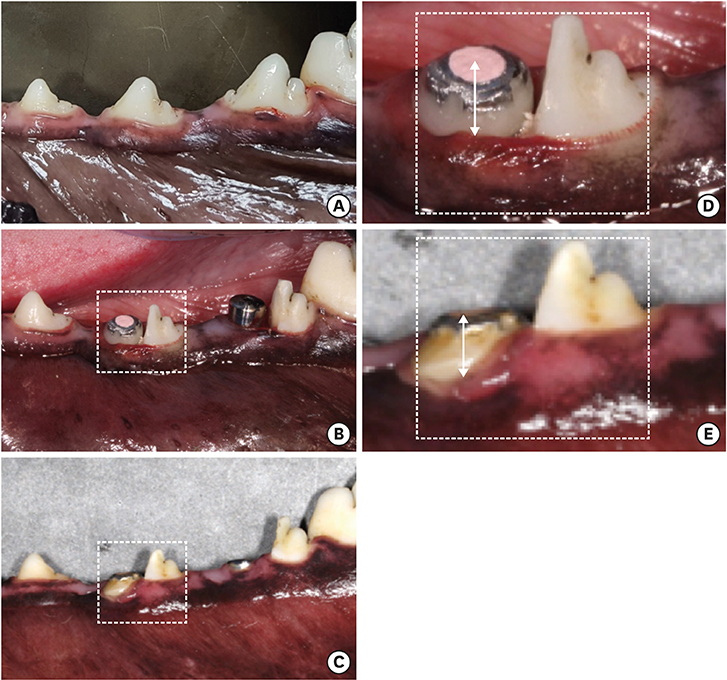
Figure 1 Clinical case from the IA and SA treatment groups at (A) baseline (before tooth extraction), (B) post-implant placement, and at (C) sacrifice. The dashed-line rectangle shows the P3 site corresponding to group IA at (D) post-implant placement and (E) sacrifice. The line with arrows shows the distance from the top of the healing abutment to the margo mucosae on the buccal side of the implant.

Figure 2 Histological slides of all 4 groups (control, SA, IA, and IAG) at sacrifice. (A) The first bone-to-implant contact on the buccal side. (B) The buccal bone crest or the most coronal location of bone substitute particles. (C) The implant shoulder on the buccal side. (D) The most coronal level of the margo mucosae on the buccal side. (E) The lingual bone crest. SA: alloplastic bone substitute material + standardized healing abutment, IA: alloplastic bone substitute material + individualized healing abutment, IAG: alloplastic bone substitute material + individualized healing abutment + a subepithelial connective tissue graft.
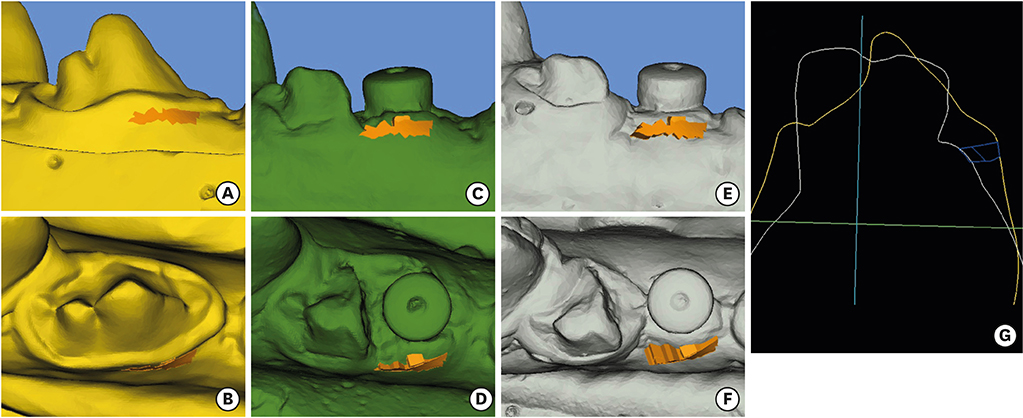
Figure 3 Digital analysis of surface scans at (A, B) baseline, (C, D) post-implant placement, and (E, F) sacrifice at an implant site from the control group. The orange rectangle corresponds to the area of interest, measuring the overall volume change defined in that region. (G) The volume of interest in a sagittal 2-dimensional cut between baseline and sacrifice.
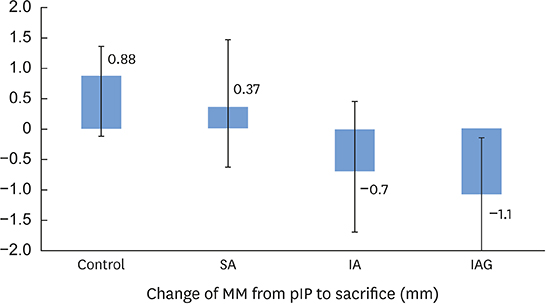
Figure 4 Mean clinical changes of the level of the buccal MM in relation to the healing abutment from pIP to sacrifice in all 4 treatment groups. SA: alloplastic bone substitute material + standardized healing abutment, IA: alloplastic bone substitute material + individualized healing abutment, IAG: alloplastic bone substitute material + individualized healing abutment + a subepithelial connective tissue graft, MM: margo mucosae, pIP: post-implant placement.

Figure 5 Histological slide with vertical measurements. MM: margo mucosae, IS: implant shoulder, BC lingual: bone crest lingual, fBIC: first bone-to-implant contact, D1: distance from MM to IS, D2: distance from MM to BC lingual, D3: distance from MM to fBIC.

Figure 6 Mean histological distance from the MM to the bBCor the most coronal location of bone substitute particles at sacrifice in all 4 treatment groups. SA: alloplastic bone substitute material + standardized healing abutment, IA: alloplastic bone substitute material + individualized healing abutment, IAG: alloplastic bone substitute material + individualized healing abutment + a subepithelial connective tissue graft, MM: margo mucosae, bBC: buccal bone crest.
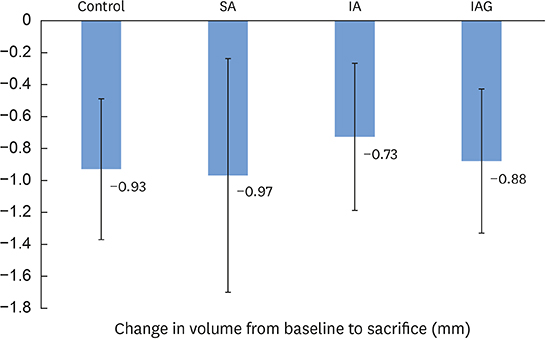
Figure 7 Mean volume change between baseline and sacrifice in all 4 treatment groups. SA: alloplastic bone substitute material + standardized healing abutment, IA: alloplastic bone substitute material + individualized healing abutment, IAG: alloplastic bone substitute material + individualized healing abutment + a subepithelial connective tissue graft.
Reference
-
1. Lang NP, Pun L, Lau KY, Li KY, Wong MC. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. Clin Oral Implants Res. 2012; 23:Suppl 5. 39–66.
Article2. Covani U, Chiappe G, Bosco M, Orlando B, Quaranta A, Barone A. A 10-year evaluation of implants placed in fresh extraction sockets: a prospective cohort study. J Periodontol. 2012; 83:1226–1234.
Article3. Hämmerle CH, Chen ST, Wilson TG Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int J Oral Maxillofac Implants. 2004; 19:Suppl. 26–28.4. Esposito M, Grusovin MG, Polyzos IP, Felice P, Worthington HV. Timing of implant placement after tooth extraction: immediate, immediate-delayed or delayed implants? A Cochrane systematic review. Eur J Oral Implantology. 2010; 3:189–205.5. Belser UC, Grütter L, Vailati F, Bornstein MM, Weber HP, Buser D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: a cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores. J Periodontol. 2009; 80:140–151.
Article6. Merheb J, Quirynen M, Teughels W. Critical buccal bone dimensions along implants. Periodontol 2000. 2014; 66:97–105.
Article7. Vignoletti F, Matesanz P, Rodrigo D, Figuero E, Martin C, Sanz M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. Clin Oral Implants Res. 2012; 23:Suppl 5. 22–38.
Article8. Chen ST, Buser D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla--a systematic review. Int J Oral Maxillofac Implants. 2014; 29:Suppl. 186–215.
Article9. Tarnow DP, Chu SJ, Salama MA, Stappert CF, Salama H, Garber DA, et al. Flapless postextraction socket implant placement in the esthetic zone: part 1. The effect of bone grafting and/or provisional restoration on facial-palatal ridge dimensional change-a retrospective cohort study. Int J Periodontics Restorative Dent. 2014; 34:323–331.
Article10. Caneva M, Botticelli D, Pantani F, Baffone GM, Rangel IG Jr, Lang NP. Deproteinized bovine bone mineral in marginal defects at implants installed immediately into extraction sockets: an experimental study in dogs. Clin Oral Implants Res. 2012; 23:106–112.
Article11. Araújo MG, Lindhe J. Socket grafting with the use of autologous bone: an experimental study in the dog. Clin Oral Implants Res. 2011; 22:9–13.
Article12. Migliorati M, Amorfini L, Signori A, Biavati AS, Benedicenti S. Clinical and aesthetic outcome with post-extractive implants with or without soft tissue augmentation: a 2-year randomized clinical trial. Clin Implant Dent Relat Res. 2015; 17:983–995.
Article13. Yoshino S, Kan JY, Rungcharassaeng K, Roe P, Lozada JL. Effects of connective tissue grafting on the facial gingival level following single immediate implant placement and provisionalization in the esthetic zone: a 1-year randomized controlled prospective study. Int J Oral Maxillofac Implants. 2014; 29:432–440.
Article14. Zuiderveld EG, Meijer HJ, den Hartog L, Vissink A, Raghoebar GM. Effect of connective tissue grafting on peri-implant tissue in single immediate implant sites: A RCT. J Clin Periodontol. 2018; 45:253–264.
Article15. De Bruyn H, Raes F, Cooper LF, Reside G, Garriga JS, Tarrida LG, et al. Three-years clinical outcome of immediate provisionalization of single Osseospeed(™) implants in extraction sockets and healed ridges. Clin Oral Implants Res. 2013; 24:217–223.
Article16. Chu SJ, Salama MA, Garber DA, Salama H, Sarnachiaro GO, Sarnachiaro E, et al. Flapless postextraction socket implant placement, part 2: the effects of bone grafting and provisional restoration on peri-implant soft tissue height and thickness- a retrospective study. Int J Periodontics Restorative Dent. 2015; 35:803–809.
Article17. Cooper LF, Reside GJ, Raes F, Garriga JS, Tarrida LG, Wiltfang J, et al. Immediate provisionalization of dental implants placed in healed alveolar ridges and extraction sockets: a 5-year prospective evaluation. Int J Oral Maxillofac Implants. 2014; 29:709–717.
Article18. Kilkenny C, Browne W, Cuthill IC, Emerson M, Altman DG. National Centre for the Replacement, Refinement and Reduction of Amimals in Research. Animal research: reporting in vivo experiments--the ARRIVE guidelines. J Cereb Blood Flow Metab. 2011; 31:991–993.
Article19. De Rouck T, Collys K, Wyn I, Cosyn J. Instant provisionalization of immediate single-tooth implants is essential to optimize esthetic treatment outcome. Clin Oral Implants Res. 2009; 20:566–570.
Article20. Cooper LF, Raes F, Reside GJ, Garriga JS, Tarrida LG, Wiltfang J, et al. Comparison of radiographic and clinical outcomes following immediate provisionalization of single-tooth dental implants placed in healed alveolar ridges and extraction sockets. Int J Oral Maxillofac Implants. 2010; 25:1222–1232.21. Quirynen M, Bollen CM, Papaioannou W, Van Eldere J, van Steenberghe D. The influence of titanium abutment surface roughness on plaque accumulation and gingivitis: short-term observations. Int J Oral Maxillofac Implants. 1996; 11:169–178.22. Quirynen M, van der Mei HC, Bollen CM, Schotte A, Marechal M, Doornbusch GI, et al. An in vivo study of the influence of the surface roughness of implants on the microbiology of supra- and subgingival plaque. J Dent Res. 1993; 72:1304–1309.
Article23. Welander M, Abrahamsson I, Berglundh T. The mucosal barrier at implant abutments of different materials. Clin Oral Implants Res. 2008; 19:635–641.
Article24. Abrahamsson I, Berglundh T, Glantz PO, Lindhe J. The mucosal attachment at different abutments. An experimental study in dogs. J Clin Periodontol. 1998; 25:721–727.
Article25. Dahlin C, Obrecht M, Dard M, Donos N. Bone tissue modelling and remodelling following guided bone regeneration in combination with biphasic calcium phosphate materials presenting different microporosity. Clin Oral Implants Res. 2015; 26:814–822.
Article26. Schmidlin PR, Nicholls F, Kruse A, Zwahlen RA, Weber FE. Evaluation of moldable, in situ hardening calcium phosphate bone graft substitutes. Clin Oral Implants Res. 2013; 24:149–157.
Article27. Yip I, Ma L, Mattheos N, Dard M, Lang NP. Defect healing with various bone substitutes. Clin Oral Implants Res. 2015; 26:606–614.
Article28. Kakar A, Rao BH, Hegde S, Deshpande N, Lindner A, Nagursky H, et al. Ridge preservation using an in situ hardening biphasic calcium phosphate (β-TCP/HA) bone graft substitute-a clinical, radiological, and histological study. Int J Implant Dent. 2017; 3:25.
Article29. Lückerath W, Röder L, Enkling N. The effect of primary stabilization of the graft in a combined surgical and prosthodontic ridge preservation protocol: a prospective controlled clinical pilot study. Int J Periodontics Restorative Dent. 2018; 38:e49–58.
Article30. Favero V, Lang NP, Canullo L, Urbizo Velez J, Bengazi F, Botticelli D. Sinus floor elevation outcomes following perforation of the Schneiderian membrane. An experimental study in sheep. Clin Oral Implants Res. 2016; 27:233–240.
Article31. Naenni N, Bienz SP, Jung RE, Hämmerle CH, Thoma DS. Histologic analyses of flapless ridge preservation in sockets with buccal dehiscence defects using two alloplastic bone graft substitutes. Clin Oral Investig. 2019.
Article32. Raes F, Cosyn J, Crommelinck E, Coessens P, De Bruyn H. Immediate and conventional single implant treatment in the anterior maxilla: 1-year results of a case series on hard and soft tissue response and aesthetics. J Clin Periodontol. 2011; 38:385–394.
Article33. Blanco J, Nuñez V, Aracil L, Muñoz F, Ramos I. Ridge alterations following immediate implant placement in the dog: flap versus flapless surgery. J Clin Periodontol. 2008; 35:640–648.
Article34. Chen ST, Darby IB, Reynolds EC, Clement JG. Immediate implant placement postextraction without flap elevation. J Periodontol. 2009; 80:163–172.
Article35. Fickl S, Kebschull M, Schupbach P, Zuhr O, Schlagenhauf U, Hürzeler MB. Bone loss after full-thickness and partial-thickness flap elevation. J Clin Periodontol. 2011; 38:157–162.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Soft and Hard Tissue Augmentation with/without Polydeoxyribonucleotide for Horizontal Ridge Deficiency: A Pilot Study in a Dog Model
- Immediate implant placement in conjunction with guided bone regeneration and/or connective tissue grafts: an experimental study in canines
- The effects of tissue punch diameter on healing around implants in flapless implant surgery
- Effects of electrical stimulation on healing of endo-osseous titanium implants in circumferential defect
- Regeneration of emergence profile with soft tissue graft and wide computer aided design/computer aided mamufacturing abutments: a clinical report
