Necrosis of Hepatocellular Carcinoma Caused by Iatrogenic Hepatic Artery Dissection during Transcatheter Arterial Chemoembolization
- Affiliations
-
- 1Department of Radiology, Inje University, Ilsan Paik Hospital, Goyang, Korea.
- 2Department of Radiology, Hallym University Dongtan Sacred Heart Hospital, Hwaseong, Korea. sheen@hallym.or.kr
- KMID: 2454036
- DOI: http://doi.org/10.3348/jksr.2019.80.3.562
Abstract
- Transcatheter arterial chemoembolization (TACE) improves the survival rate in patients with hepatocellular carcinoma (HCC). Despite the low probability, iatrogenic hepatic arterial dissections during interventional procedure are rarely created by the technical difficulties. Direct trauma from the guidewire, the tip of the catheter, or the jet of contrast injection can contribute to iatrogenic hepatic arterial dissections. We report one case of a female who had HCC necrosis caused by iatrogenic hepatic arterial dissection during TACE. Ischemia resulting from iatrogenic hepatic arterial dissection during TACE was smilar to the result of transarterial embolization for HCC on our case. To our knowledge, none of the similar cases was reported in previously published literatures.
MeSH Terms
Figure
-
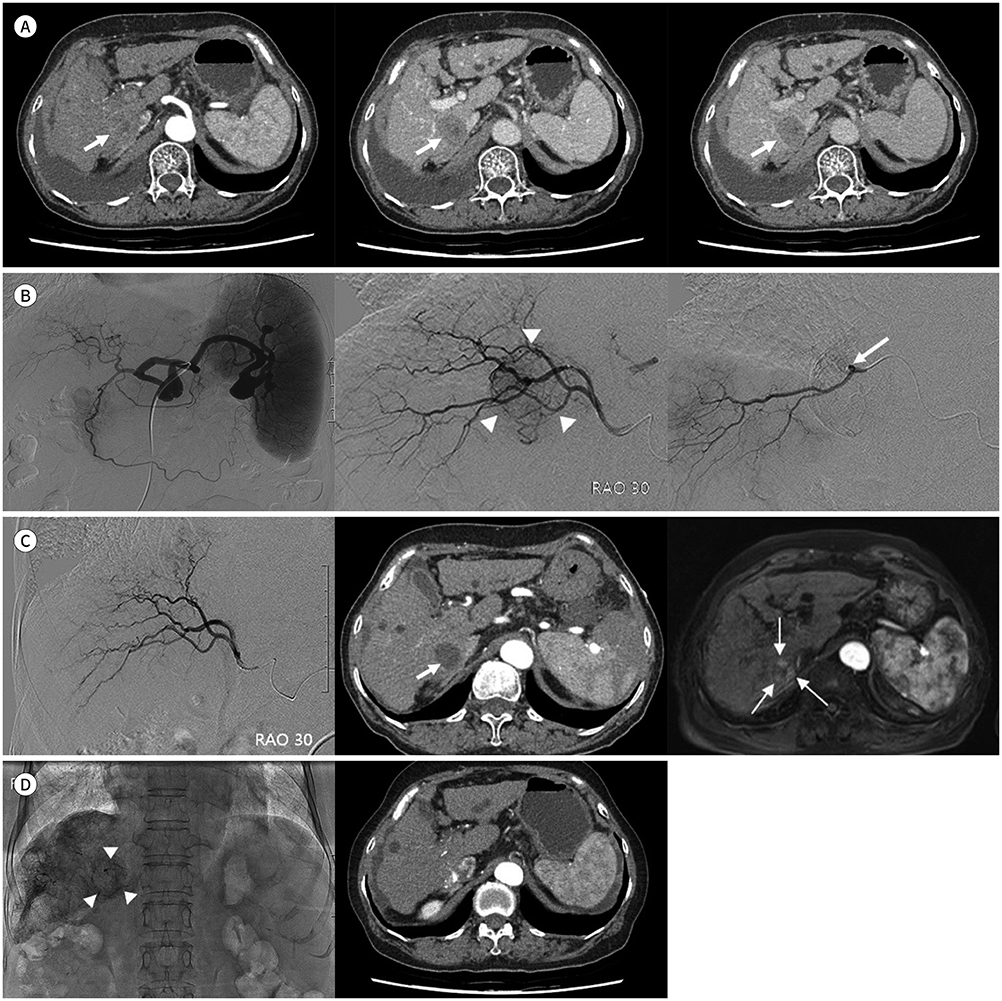
Fig. 1 Necrosis of HCC caused by iatrogenic hepatic artery dissection during TACE in a 67-year old female patient. A. Three-phase abdominal CT shows a nodular lesion with subtle centripetal arterial enhancement and portal/delayed wash-out is between S6 and S7, compatible with HCC (3.0 × 2.5 cm, arrows). B. Celiac angiography shows a tumor staining in right hepatic lobe of liver with several aneurysms in splenic artery. Posterior divisional HA angiography shows arterial staining target lesion feeding from A7 (arrowheads). After trying to advance microcatheter into A7, angiography shows no arterial flow to A7 due to HA dissection. The previous staining target lesion is no longer visible (arrow). C. One month later, posterior divisional HA angiography shows recanalization of previously dissected A7 without tumor staining, making us suspend TACE. Three-phase abdomen CT immediately taken after angiography shows HCC necrosis with decrease in size (2.5 × 2.2 cm) (thick arrow). Follow-up liver MRI taken two months after the event of HCC necrosis shows HCC recurrence along the margin of HCC necrosis (thin arrows). D. Segmentally selective TACE via A7 was done for recurred HCC, and the procedure ended after confirming the lipiodol uptake (arrowheads). The latest follow-up 3-phase abdomen CT shows partial lipiodol uptake around the HCC without the evidence of arterial enhancing viable tumor. A7 = hepatic arterial branch for Couinaud's segment VII, HA = hepatic artery, HCC = hepatocellular carcinoma, S6 = Couinaud's segment VI, S7 = Couinaud's segment VII, TACE = transcatheter arterial chemoembolization
Reference
-
1. Chuang VP, Wallace S. Hepatic artery embolization in the treatment of hepatic neoplasms. Radiology. 1981; 140:51–58.
Article2. Jung E, Shin JH, Kim JH, Yoon HK, Ko GY, Sung KB. Arterial dissections during transcatheter arterial chemoembolization for hepatocellular carcinoma: a 19-year clinical experience at a single medical institution. Acta Radiol. 2016; 58:842–848.
Article3. Yoon DY, Park JH, Chung JW, Han JK, Han MC. Iatrogenic dissection of the celiac artery and its branches during transcatheter arterial embolization for hepatocellular carcinoma: outcome in 40 patients. Cardiovasc Intervent Radiol. 1995; 18:16–19.
Article4. Finch IJ. Use of the palmaz stent in ostial celiac artery stenosis. J Vasc Interv Radiol. 1992; 3:633–635.
Article5. Marelli L, Stigliano R, Triantos C, Senzolo M, Cholongitas E, Davies N, et al. Transarterial therapy for hepatocellular carcinoma: which technique is more effective? A systematic review of cohort and randomized studies. Cardiovasc Intervent Radiol. 2007; 30:6–25.
Article6. Maeda N, Osuga K, Mikami K, Higashihara H, Onishi H, Nakaya Y, et al. Angiographic evaluation of hepatic arterial damage after transarterial chemoembolization for hepatocellular carcinoma. Radiat Med. 2008; 26:206–212.
Article7. Sueyoshi E, Hayashida T, Sakamoto I, Uetani M. Vascular complications of hepatic artery after transcatheter arterial chemoembolization in patients with hepatocellular carcinoma. AJR Am J Roentgenol. 2010; 195:245–251.
Article8. Yoshimitsu K. Transarterial chemoembolization using iodized oil for unresectable hepatocellular carcinoma: perspective from multistep hepatocarcinogenesis. Hepat Med. 2014; 6:89–94.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An ischemic skin lesion after chemoembolization of the right internal mammary artery in a patient with hepatocellular carcinoma
- Efficacy of Hepatic Arterial Infusion Chemotherapy and Radiofrequency Ablation against Hepatocellular Carcinoma Refractory to Transarterial Chemoembolization and Vascular Variation: A Case Study
- Supraumbilical Skin Rash as a Rare Complication of Transcatheter Arterial Chemoembolization in Patients with Hepatocellular Carcinoma
- Hepatocellular Carcinoma Extending to the Inferior Vena Cava and Right Atrium-A Case Report of 4 Years Survival after Repeated Transcatheter Arterial Chemoembolization Therapy -
- Rupture of Hepatocellular Carcinoma Following Transcatheter Arterial Chemoembolization: A Case Report
