Radiologic Report for Magnetic Resonance Imaging of Rectal Cancer before Treatment
- Affiliations
-
- 1Department of Radiology, School of Medicine, Kyungpook National University, Kyungpook National University Chilgok Hospital, Daegu, Korea. shcho2405@gmail.com
- KMID: 2454024
- DOI: http://doi.org/10.3348/jksr.2019.80.3.425
Abstract
- Modern management of rectal cancer highly depends on the interpretation of high-spatial-resolution MRI, which determines the benefits from preoperative chemoradiotherapy or surgery alone. Accordingly, the baseline MRI report plays a pivotal role in planning the treatment. Although several structured reporting templates for rectal cancer staging on MRI are available, many radiologists still use the free-text format. In this review, we discuss the essential items for reporting rectal cancer on MRI before treatment to guide general radiologists in preparing a qualified report.
Figure
-
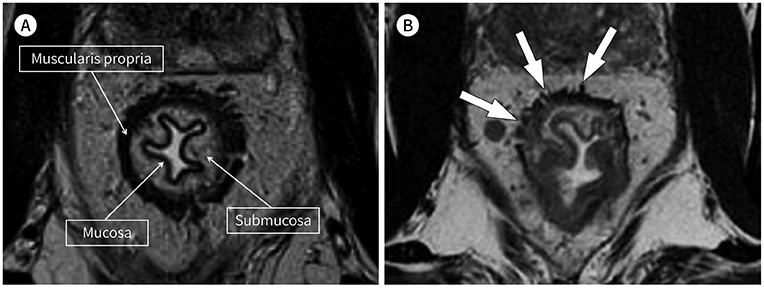
Fig. 1 Rectal anatomy on magnetic resonance imaging. A. The three layers of the rectum wall (arrows). B. Normal saw-tooth appearance of the anterior longitudinal muscle in the lower rectum (arrows).
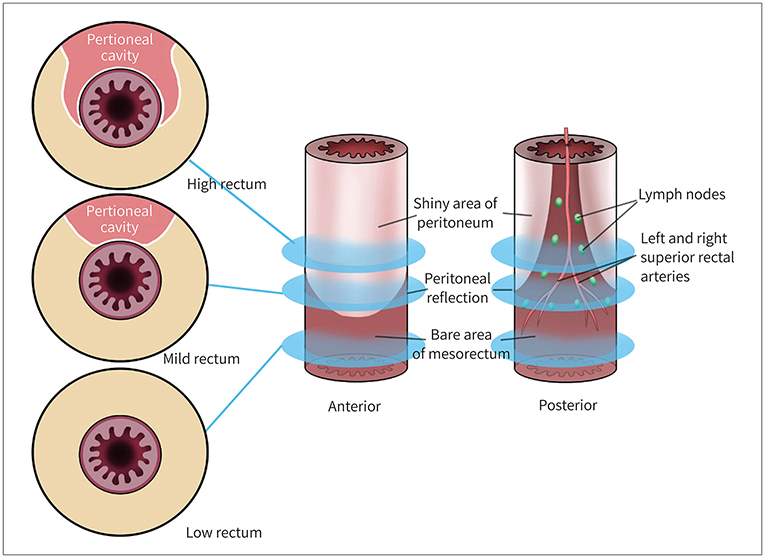
Fig. 2 The rectal peritoneum.
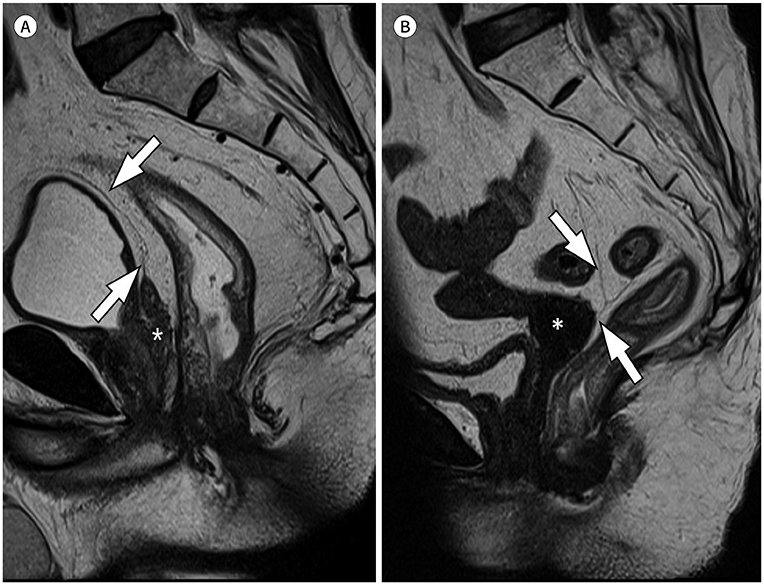
Fig. 3 Anterior peritoneal reflection on magnetic resonance imaging. A. In men, the anterior peritoneal reflecion (arrows) is located just above the tip of the seminal vesicle (asterisk). B. In women, the anterior peritoneal reflecion (arrows) is located at the level of the uterine cervix (asterisk).
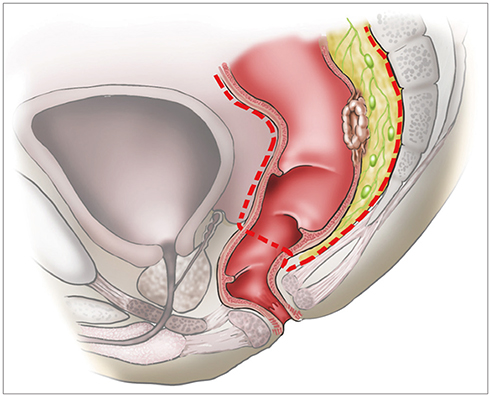
Fig. 4 Extent of total mesorectal excision.
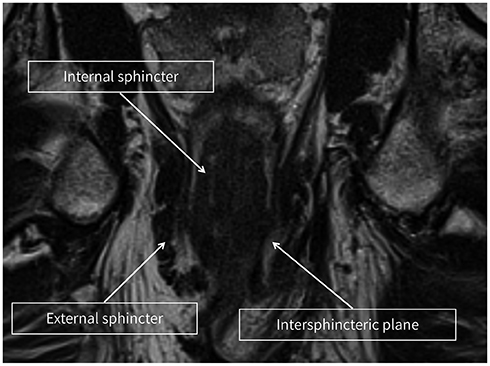
Fig. 5 Anatomy of sphincter complex (arrows).
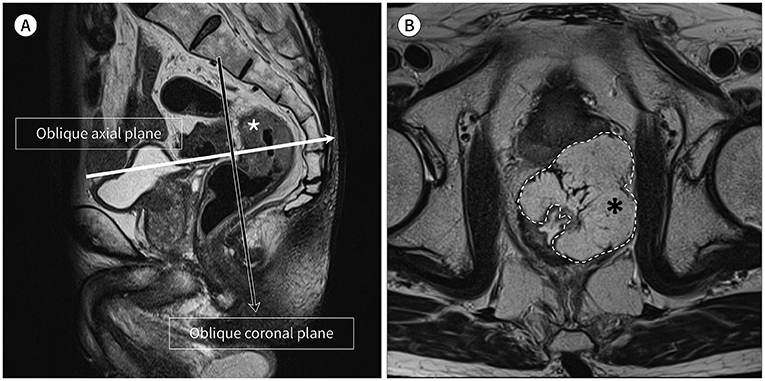
Fig. 6 Magnetic resonance imaging protocol. A. Oblique axial and coronal images are obtained orthogonal (white arrow) or parallel (black arrow) to the long axis of the tumor (asterisk). B. Mucinous lower rectal cancer (asterisk). Oblique axial T2-weighted image with high-resolution and small field-of-view is recommended (an example from our institution: 3 mm slice thickness, 160 mm × 160 mm field-of-view, 256 × 256 pixels, 4–6 excitations, 1.1 mm3 voxel resolution).
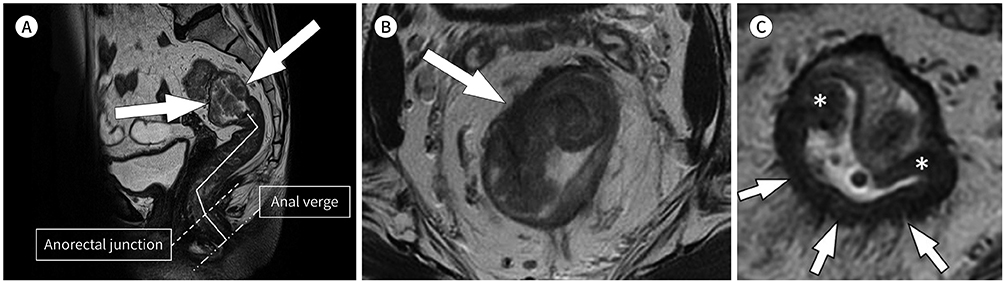
Fig. 7 Tumor height and morphology. A. Distances from the anal verge and anorectal junction to the distal margin of the tumor (arrows) by a curvilinear measurement (straight line) along the luminal center. B. Polypoid mass with the fibrovascular stalk (arrow) at 11 o'clock position. C. Semi-annular wall thickening with an invasive edge (arrows) at 4–9 o'clock position and two raised rolled edges (asterisks) at 3 and 9 o'clock positions.
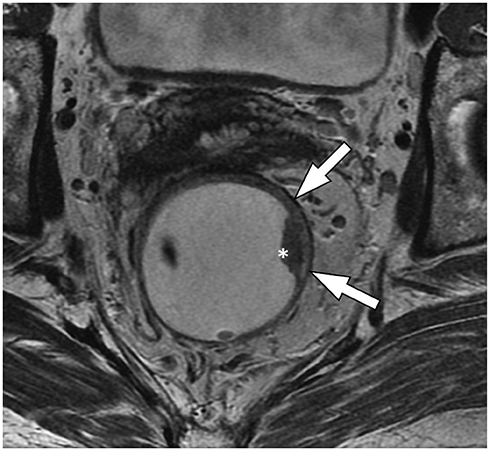
Fig. 8 T1 rectal cancer (asterisks) with preserved high-signal stripe of the submucosal layer (arrows).
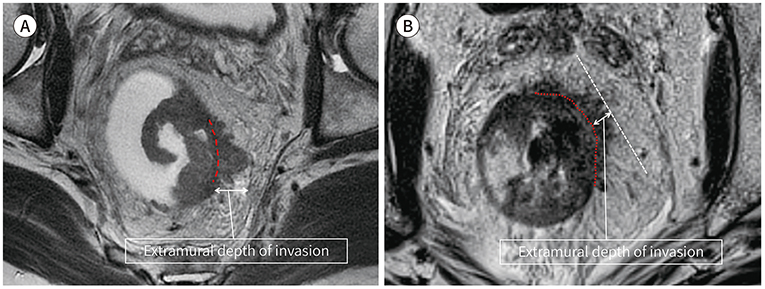
Fig. 9 T3 substage. A. Nodular extramural extension. Extramural depth of invasion (arrow) measured by the distance from imaginary line (dashed line) of outer margin for muscularis propria layer to outer margin of tumor. B. Broad-base bulging extramural extension. Extramural depth of invasion (arrow) measured by the distance from imaginary line (red dashed line) of outer margin for muscularis propria layer to outer margin of tumor (white dashed line).
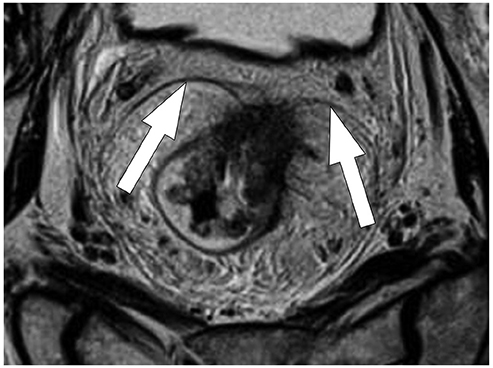
Fig. 10 T4a rectal cancer with anterior peritoneal reflection (arrows) invasion.
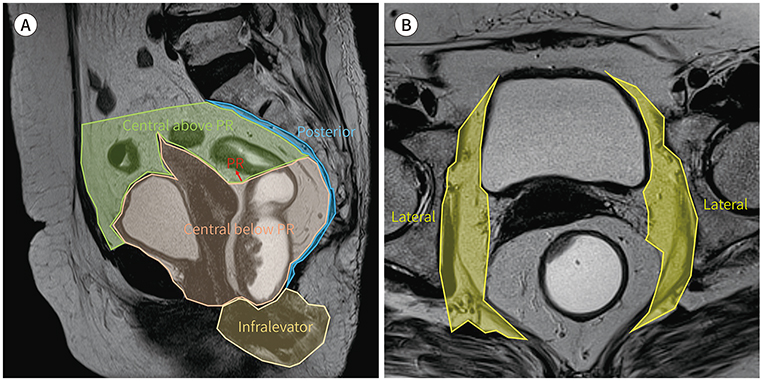
Fig. 11 Compartments of the pelvis. A. Sagittal image shows central compartments above/below the PR (arrow), posterior compartment, and infralevator compartment. B. Oblique axial image shows the lateral compartment. PR = peritoneal reflection.
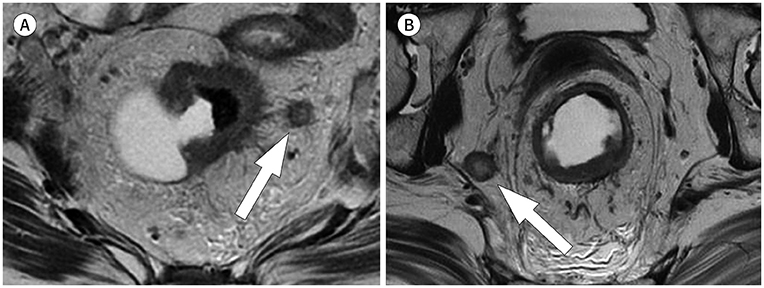
Fig. 12 Lymph node evaluation. A. A 9 mm metastatic mesorectal node with round, irregular margin and internal heterogeneity (arrow). B. A 13 mm metastatic internal iliac node with round and internal heterogeneity (arrow).
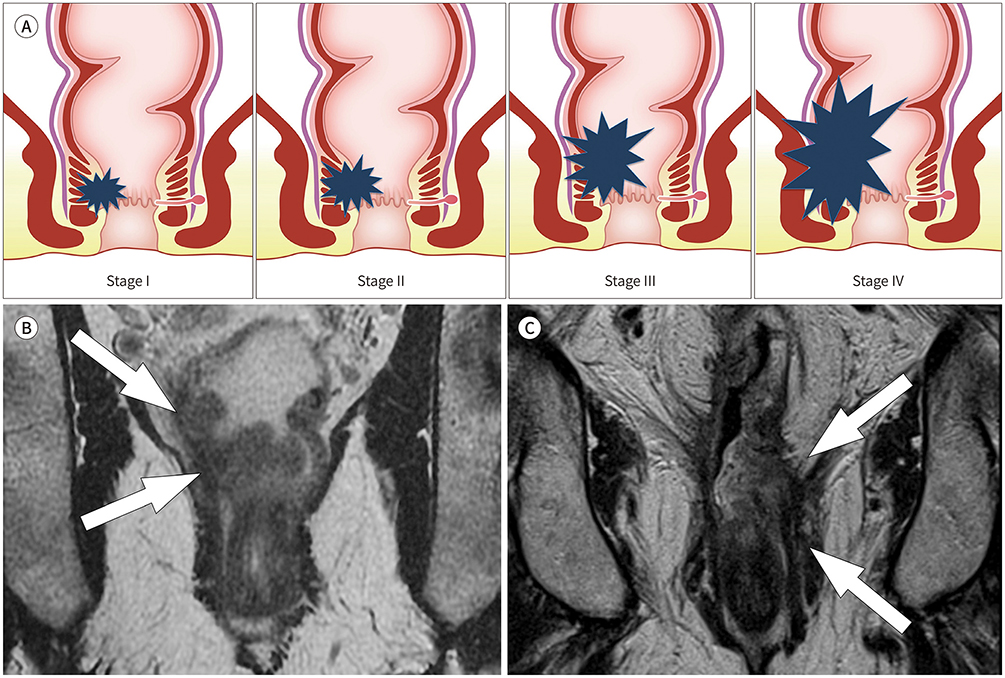
Fig. 13 Sphincter complex. A. Illustration of magnetic resonance image staging of lower rectal cancer. B. Stage I: lower rectal cancer (arrows) is confined to the bowel wall. C. Stage IV: lower rectal cancer (arrows) invades the intersphincteric plane and left levator ani muscle.
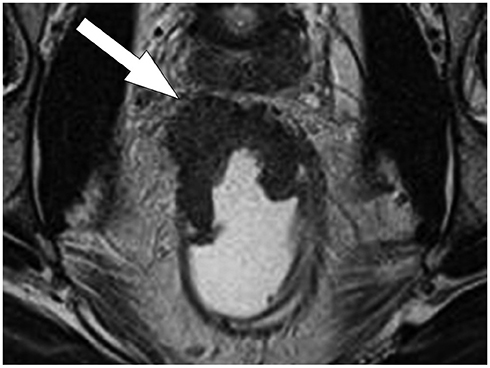
Fig. 14 Circumferential resection margin. “Involved” mesorectal fascia at 10–11 o'clock position by direct spreading of the primary tumor (arrow).
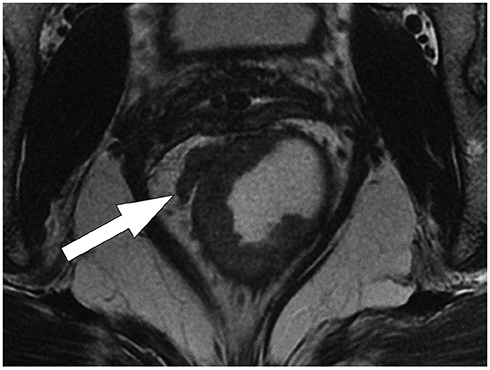
Fig. 15 Extramural venous invasion. Intermediate tumor signal intensity within the marginated, expanded extramural nodular vein contiguous to the primary tumor (arrow).
Reference
-
1. Ferlay J, Colombet M, Soerjomataram I, Mathers C, Parkin D, Piñeros M, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019; 144:1941–1953.2. Korean Statistical Information Service. Cancer registration statistics. 2019. Accessed May 1, 2019. Available at. http://kosis.kr/statisticsList/statisticsList_01List.jsp.3. Engelen SM, Maas M, Lahaye MJ, Leijtens JW, Van Berlo CL, Jansen RL, et al. Modern multidisciplinary treatment of rectal cancer based on staging with magnetic resonance imaging leads to excellent local control, but distant control remains a challenge. Eur J Cancer. 2013; 49:2311–2320.4. Kapiteijn E, Marijnen CA, Nagtegaal ID, Putter H, Steup WH, Wiggers T, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med. 2001; 345:638–646.5. Tong T, Gollub MJ. Prognostic stratification by extramural depth of tumor invasion of primary rectal cancer based on the Radiological Society of North America. AJR Am J Roentgenol. 2014; 203:W749.6. Wheeler JM, Dodds E, Warren BF, Cunningham C, George BD, Jones AC, et al. Preoperative chemoradiotherapy and total mesorectal excision surgery for locally advanced rectal cancer: correlation with rectal cancer regression grade. Dis Colon Rectum. 2004; 47:2025–2031.7. Kennedy ED, Milot L, Fruitman M, Al-Sukhni E, Heine G, Schmocker S, et al. Development and implementation of a synoptic MRI report for preoperative staging of rectal cancer on a population-based level. Dis Colon Rectum. 2014; 57:700–708.8. Tersteeg JJC, Gobardhan PD, Crolla RMPH, Kint PAM, Niers-Stobbe I, Boonman-de Winter LJM, et al. Improving the quality of MRI reports of preoperative patients with rectal cancer: effect of national guidelines and structured reporting. AJR Am J Roentgenol. 2018; 210:1240–1244.9. Benson AB 3rd, Venook AP, Al-Hawary MM, Cederquist L, Chen YJ, Ciombor KK, et al. Rectal cancer, version 2.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2018; 16:874–890.10. Gollub MJ, Maas M, Weiser M, Beets GL, Goodman K, Berkers L, et al. Recognition of the anterior peritoneal reflection at rectal MRI. AJR Am J Roentgenol. 2013; 200:97–101.11. Park JG. Coloproctology. 4th ed. Seoul: Iljogak;2012. p. 25–66.12. Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986; 1:1479–1482.13. Sauer R, Becker H, Hohenberger W, Rödel C, Wittekind C, Fietkau R, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004; 351:1731–1740.14. Patel UB, Brown G, Rutten H, West N, Sebag-Montefiore D, Glynne-Jones R, et al. Comparison of magnetic resonance imaging and histopathological response to chemoradiotherapy in locally advanced rectal cancer. Ann Surg Oncol. 2012; 19:2842–2852.15. Francois Y, Nemoz CJ, Baulieux J, Vignal J, Grandjean JP, Partensky C, et al. Influence of the interval between preoperative radiation therapy and surgery on downstaging and on the rate of sphincter-sparing surgery for rectal cancer: the Lyon R90-01 randomized trial. J Clin Oncol. 1999; 17:2396.16. Battersby NJ, Dattani M, Rao S, Cunningham D, Tait D, Adams R, et al. A rectal cancer feasibility study with an embedded phase III trial design assessing magnetic resonance tumour regression grade (mrTRG) as a novel biomarker to stratify management by good and poor response to chemoradiotherapy (TRIGGER): study protocol for a randomised controlled trial. Trials. 2017; 18:394.17. Brown G, Daniels IR, Richardson C, Revell P, Peppercorn D, Bourne M. Techniques and trouble-shooting in high spatial resolution thin slice MRI for rectal cancer. Br J Radiol. 2005; 78:245–251.18. Koh DM, Brown G, Temple L, Blake H, Raja A, Toomey P, et al. Distribution of mesorectal lymph nodes in rectal cancer: in vivo MR imaging compared with histopathological examination. Initial observations. Eur Radiol. 2005; 15:1650–1657.19. Kim DJ, Kim JH, Lim JS, Chung JJ, Yu JS, Kim MJ, et al. Preoperative evaluation of lower rectal cancer by pelvic MR with and without gel filling. J Korean Soc Magn Reson Med. 2014; 18:323–331.20. Stijns RC, Scheenen TW, De Wilt JH, Fütterer JJ, Beets-Tan RG. The influence of endorectal filling on rectal cancer staging with MRI. Br J Radiol. 2018; 91:20180205.21. Kim SH, Lee JM, Lee MW, Kim GH, Han JK, Choi BI. Sonography transmission gel as endorectal contrast agent for tumor visualization in rectal cancer. AJR Am J Roentgenol. 2008; 191:186–189.22. Beets-Tan RGH, Lambregts DMJ, Maas M, Bipat S, Barbaro B, Curvo-Semedo L, et al. Magnetic resonance imaging for clinical management of rectal cancer: updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur Radiol. 2018; 28:1465–1475.23. KSAR Study Group for Rectal Cancer. Essential items for structured reporting of rectal cancer MRI: 2016 consensus recommendation from the Korean Society of Abdominal Radiology. Korean J Radiol. 2017; 18:132–151.24. Kuvshinoff B, Maghfoor I, Miedema B, Bryer M, Westgate S, Wilkes J, et al. Distal margin requirements after preoperative chemoradiotherapy for distal rectal carcinomas: are < or = 1 cm distal margins sufficient? Ann Surg Oncol. 2001; 8:163–169.25. Park JS, Sakai Y, Simon NS, Law WL, Kim HR, Oh JH, et al. Long-term survival and local relapse following surgery without radiotherapy for locally advanced upper rectal cancer: an international multi-institutional study. Medicine (Baltimore). 2016; 95:e2990.26. Shepherd NA, Baxter KJ, Love SB. Influence of local peritoneal involvement on pelvic recurrence and prognosis in rectal cancer. J Clin Pathol. 1995; 48:849–855.27. Bhoday J, Balyasnikova S, Wale A, Brown G. How should imaging direct/orient management of rectal cancer? Clin Colon Rectal Surg. 2017; 30:297–312.28. Al-Sukhni E, Milot L, Fruitman M, Beyene J, Victor JC, Schmocker S, et al. Diagnostic accuracy of MRI for assessment of T category, lymph node metastases, and circumferential resection margin involvement in patients with rectal cancer: a systematic review and meta-analysis. Ann Surg Oncol. 2012; 19:2212–2223.29. Puli SR, Bechtold ML, Reddy JB, Choudhary A, Antillon MR, Brugge WR. How good is endoscopic ultrasound in differentiating various T stages of rectal cancer? Meta-analysis and systematic review. Ann Surg Oncol. 2009; 16:254–265.30. Taylor FG, Quirke P, Heald RJ, Moran B, Blomqvist L, Swift I, et al. Preoperative high-resolution magnetic resonance imaging can identify good prognosis stage I, II, and III rectal cancer best managed by surgery alone: a prospective, multicenter, European study. Ann Surg. 2011; 253:711–719.31. Merkel S, Mansmann U, Siassi M, Papadopoulos T, Hohenberger W, Hermanek P. The prognostic inhomogeneity in pT3 rectal carcinomas. Int J Colorectal Dis. 2001; 16:298–304.32. Gollub MJ, Arya S, Beets-Tan RG, DePrisco G, Gonen M, Jhaveri K, et al. Use of magnetic resonance imaging in rectal cancer patients: Society of Abdominal Radiology (SAR) rectal cancer disease-focused panel (DFP) recommendations 2017. Abdom Radiol (NY). 2018; 43:2893–2902.33. Hermanek P, Henson DE, Hutter RV, Sobin LH. UICC TNM supplement 1993: a commentary on uniform use. Berlin: Springer-Verlag;1993.34. Siddiqui MRS, Simillis C, Bhoday J, Battersby NJ, Mok J, Rasheed S, et al. A meta-analysis assessing the survival implications of subclassifying T3 rectal tumours. Eur J Cancer. 2018; 104:47–61.35. Brown G, Richards CJ, Newcombe RG, Dallimore NS, Radcliffe AG, Carey DP, et al. Rectal carcinoma: thinsection MR imaging for staging in 28 patients. Radiology. 1999; 211:215–222.36. Cho SH, Kim SH, Bae JH, Jang YJ, Kim HJ, Lee D, et al. Prognostic stratification by extramural depth of tumor invasion of primary rectal cancer based on the Radiological Society of North America proposal. AJR Am J Roentgenol. 2014; 202:1238–1244.37. Park SH. Degree of error of thin-section MR in measuring extramural depth of tumor invasion in patients with rectal cancer. Radiology. 2008; 246:647. author reply 647-648.38. Georgiou PA, Tekkis PP, Constantinides VA, Patel U, Goldin RD, Darzi AW, et al. Diagnostic accuracy and value of magnetic resonance imaging (MRI) in planning exenterative pelvic surgery for advanced colorectal cancer. Eur J Cancer. 2013; 49:72–81.39. Quirke P, Steele R, Monson J, Grieve R, Khanna S, Couture J, et al. Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: a prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomised clinical trial. Lancet. 2009; 373:821–828.40. Chand M, Moran BJ, Jones RG, Heald RJ, Brown G. Lymph node status does not predict local recurrence in the total mesorectal excision era. Dis Colon Rectum. 2014; 57:127–129.41. Ruppert R, Junginger T, Ptok H, Strassburg J, Maurer CA, Brosi P, et al. Oncological outcome after MRI-based selection for neoadjuvant chemoradiotherapy in the OCUM Rectal Cancer Trial. Br J Surg. 2018; 105:1519–1529.42. Brown G, Richards CJ, Bourne MW, Newcombe RG, Radcliffe AG, Dallimore NS, et al. Morphologic predictors of lymph node status in rectal cancer with use of high-spatial-resolution MR imaging with histopathologic comparison. Radiology. 2003; 227:371–377.43. Kim JH, Beets GL, Kim MJ, Kessels AG, Beets-Tan RG. High-resolution MR imaging for nodal staging in rectal cancer: are there any criteria in addition to the size? Eur J Radiol. 2004; 52:78–83.44. Cai JH, Liu J, Ikeguch M, Yan QH, Zhou BJ, Song WQ, et al. Clinical significance of micrometastasis in lymph nodes and microinvasion in primary lesion in submucosal gastric cancer. Zhonghua Wai Ke Za Zhi. 2005; 43:161–165.45. Salerno GV, Daniels IR, Moran BJ, Heald RJ, Thomas K, Brown G. Magnetic resonance imaging prediction of an involved surgical resection margin in low rectal cancer. Dis Colon Rectum. 2009; 52:632–639.46. Shihab OC, Moran BJ, Heald RJ, Quirke P, Brown G. MRI staging of low rectal cancer. Eur Radiol. 2009; 19:643–650.47. Shihab OC, Heald RJ, Rullier E, Brown G, Holm T, Quirke P, et al. Defining the surgical planes on MRI improves surgery for cancer of the low rectum. Lancet Oncol. 2009; 10:1207–1211.48. Battersby NJ, How P, Moran B, Stelzner S, West NP, Branagan G, et al. Prospective validation of a low rectal cancer magnetic resonance imaging staging system and development of a local recurrence risk stratification model: the MERCURY II study. Ann Surg. 2016; 263:751–760.49. Nagtegaal ID, Quirke P. What is the role for the circumferential margin in the modern treatment of rectal cancer? J Clin Oncol. 2008; 26:303–312.50. Adam IJ, Mohamdee MO, Martin IG, Scott N, Finan PJ, Johnston D, et al. Role of circumferential margin involvement in the local recurrence of rectal cancer. Lancet. 1994; 344:707–711.51. Shihab OC, Quirke P, Heald RJ, Moran BJ, Brown G. Magnetic resonance imaging-detected lymph nodes close to the mesorectal fascia are rarely a cause of margin involvement after total mesorectal excision. Br J Surg. 2010; 97:1431–1436.52. Nagtegaal ID, Marijnen CA, Kranenbarg EK, Van de Velde CJ, Van Krieken JH. Pathology Review Committee. Cooperative Clinical Investigators. Circumferential margin involvement is still an important predictor of local recurrence in rectal carcinoma: not one millimeter but two millimeters is the limit. Am J Surg Pathol. 2002; 26:350–357.53. Xie H, Zhou X, Zhuo Z, Che S, Xie L, Fu W. Effectiveness of MRI for the assessment of mesorectal fascia involvement in patients with rectal cancer: a systematic review and meta-analysis. Dig Surg. 2014; 31:123–134.54. Chand M, Siddiqui MR, Swift I, Brown G. Systematic review of prognostic importance of extramural venous invasion in rectal cancer. World J Gastroenterol. 2016; 22:1721–1726.55. Chand M, Palmer T, Blomqvist L, Nagtegaal I, West N, Brown G. Evidence for radiological and histopathological prognostic importance of detecting extramural venous invasion in rectal cancer: recommendations for radiology and histopathology reporting. Colorectal Dis. 2015; 17:468–473.56. Siddiqui MRS, Simillis C, Hunter C, Chand M, Bhoday J, Garant A, et al. A meta-analysis comparing the risk of metastases in patients with rectal cancer and MRI-detected extramural vascular invasion (mrEMVI) vs mrEMVI-negative cases. Br J Cancer. 2017; 116:1513–1519.57. Bae JS, Kim SH, Hur BY, Chang W, Park J, Park HE, et al. Prognostic value of MRI in assessing extramural venous invasion in rectal cancer: multi-readers' diagnostic performance. Eur Radiol. 2019; 01. 07. DOI: 10.1007/s00330-018-5926-9. [Epub]. Available at. .58. Jhaveri KS, Hosseini-Nik H, Thipphavong S, Assarzadegan N, Menezes RJ, Kennedy ED, et al. MRI detection of extramural venous invasion in rectal cancer: correlation with histopathology using elastin stain. AJR Am J Roentgenol. 2016; 206:747–755.59. Smith NJ, Barbachano Y, Norman AR, Swift RI, Abulafi AM, Brown G. Prognostic significance of magnetic resonance imaging-detected extramural vascular invasion in rectal cancer. Br J Surg. 2008; 95:229–236.60. Sohn B, Lim JS, Kim H, Myoung S, Choi J, Kim NK, et al. MRI-detected extramural vascular invasion is an independent prognostic factor for synchronous metastasis in patients with rectal cancer. Eur Radiol. 2015; 25:1347–1355.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Imaging Diagnosis of Colorectal Cancer
- Rectal Syphilis Mimicking Malignancy: A Case Report
- US and MRI Findings of Penile Metastasis from Rectal Adenocarcinoma: A Case Report
- Clinical Significance of Preoperative Magnetic Resonance Imaging in Staging of Rectal Cancer
- Imaging Diagnosis of Locally Advanced Rectal Cancer: Tumor Staging before and after Preoperative Chemoradiotherapy
