J Gastric Cancer.
2019 Jun;19(2):157-164. 10.5230/jgc.2019.19.e12.
Prospective Multicenter Feasibility Study of Laparoscopic Sentinel Basin Dissection after Endoscopic Submucosal Dissection for Early Gastric Cancer: SENORITA 2 Trial Protocol
- Eom BW

- Yoon HM
- Min JS
- Cho I
- Park JH
- Jung MR
- Hur H
- Kim YW
- Park YK
- Nam BH
- Ryu KW
- Sentinel Node Oriented Tailored Approach (SENORITA) Study Group
- Affiliations
-
- 1Center for Gastric Cancer, Research Institute and Hospital, National Cancer Center, Goyang, Korea. docryu@ncc.re.kr
- 2Department of Surgery, Dongnam Institute of Radiological and Medical Science, Busan, Korea.
- 3Department of Surgery, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 4Department of Surgery, Gyeongsang National University, Jinju, Korea.
- 5Department of Surgery, Chonnam National University Hwasun Hospital, Hwasun, Korea.
- 6Department of Surgery, Ajou University School of Medicine, Suwon, Korea.
- 7Biometric Research Branch, Research Institute for National Cancer Control & Evaluation, National Cancer Center, Goyang, Korea.
- KMID: 2449936
- DOI: http://doi.org/10.5230/jgc.2019.19.e12
Abstract
- PURPOSE
Although standard radical gastrectomy is recommended after noncurative resection of endoscopic submucosal dissection (ESD) for early gastric cancer in most cases, residual tumor and lymph node metastasis have not been identified after surgery. The aim of this study is to evaluate the feasibility of sentinel node navigation surgery after noncurative ESD.
MATERIALS AND METHODS
This trial is an investigator-initiated, multicenter prospective phase II trial. Patients who underwent ESD for clinical stage T1N0M0 gastric cancer with noncurative resections were eligible. Qualified investigators who completed the prior phase III trial (SENORITA 1) are exclusively allowed to participate. In this study, 2 detection methods will be used: 1) intraoperative endoscopic submucosal injection of dual tracer, including radioisotope and indocyanine green (ICG) with sentinel basins detected using gamma-probe; 2) endoscopic injection of ICG, with sentinel basins detected using a fluorescence imaging system. Standard laparoscopic gastrectomy with lymphadenectomy will be performed. Sample size is calculated based on the inferior confidence interval of the detection rate of 95%, and the calculated accrual is 237 patients. The primary endpoint is detection rate, and the secondary endpoints are sensitivity and postoperative complications.
CONCLUSIONS
This study is expected to clarify the feasibility of laparoscopic sentinel basin dissection after noncurative ESD. If the feasibility is demonstrated, a multicenter phase III trial will be initiated to compare laparoscopic sentinel node navigation surgery versus laparoscopic standard gastrectomy in early gastric cancer after endoscopic resection. TRIAL REGISTRATION: ClinicalTrials.gov Identifier: NCT03123042
MeSH Terms
Figure
-
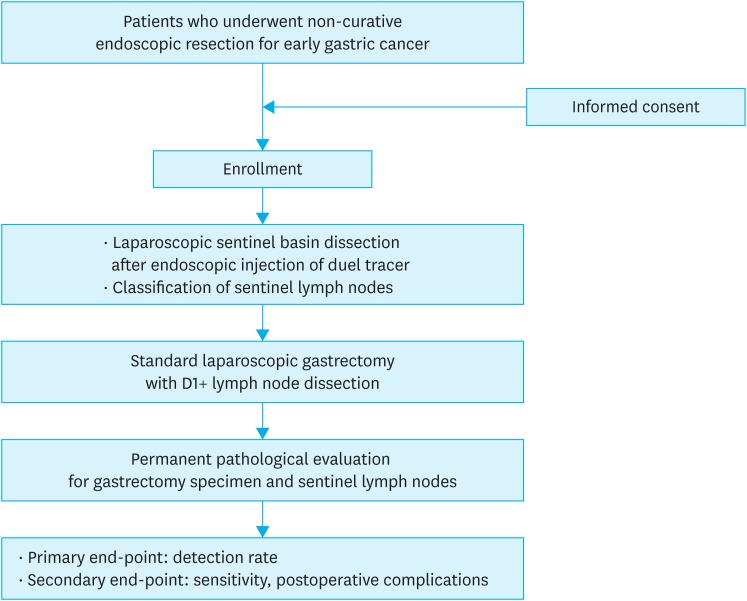
Fig. 1 Study scheme of the SENORITA 2 trial.SENORITA = Sentinel Node Oriented Tailored Approach.
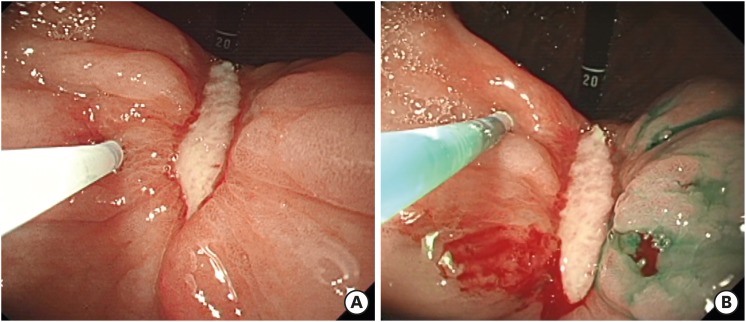
Fig. 2 First endoscopic injection of dual tracer around the ESD ulcer scar (A). Final endoscopic injection around the ESD ulcer scar. Elevated mucosa around the ESD scar by tracer injection is observed (B).ESD = endoscopic submucosal dissection.

Fig. 3 Intraoperative identification of sentinel basins. Green-stained basin after injection of dual tracer (A) and indocyanine green fluorescence imaging (B-D). Lymphatic vessels draining the tumor and sentinel node are visualized by green (B), blue (C), and bright fluorescence (D).
Reference
-
1. Wang Z, Dong ZY, Chen JQ, Liu JL. Diagnostic value of sentinel lymph node biopsy in gastric cancer: a meta-analysis. Ann Surg Oncol. 2012; 19:1541–1550. PMID: 22048632.
Article2. Kitagawa Y, Takeuchi H, Takagi Y, Natsugoe S, Terashima M, Murakami N, et al. Sentinel node mapping for gastric cancer: a prospective multicenter trial in Japan. J Clin Oncol. 2013; 31:3704–3710. PMID: 24019550.
Article3. Park JY, Kim YW, Ryu KW, Nam BH, Lee YJ, Jeong SH, et al. Assessment of laparoscopic stomach preserving surgery with sentinel basin dissection versus standard gastrectomy with lymphadenectomy in early gastric cancer-a multicenter randomized phase III clinical trial (SENORITA trial) protocol. BMC Cancer. 2016; 16:340. PMID: 27246120.
Article4. Eom BW, Jung KW, Won YJ, Yang H, Kim YW. Trends in gastric cancer incidence according to the clinicopathological characteristics in Korea, 1999–2014. Cancer Res Treat. 2018; 50:1343–1350. PMID: 29361823.
Article5. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011; 14:113–123. PMID: 21573742.6. Eom BW, Kim YI, Kim KH, Yoon HM, Cho SJ, Lee JY, et al. Survival benefit of additional surgery after noncurative endoscopic resection in patients with early gastric cancer. Gastrointest Endosc. 2017; 85:155–163.e3. PMID: 27460389.
Article7. Kim ER, Lee H, Min BH, Lee JH, Rhee PL, Kim JJ, et al. Effect of rescue surgery after non-curative endoscopic resection of early gastric cancer. Br J Surg. 2015; 102:1394–1401. PMID: 26313295.
Article8. Ishii S, Yamashita K, Kato H, Nishizawa N, Ushiku H, Mieno H, et al. Predictive factors for lymph node metastasis in additional gastrectomy after endoscopic resection of cT1aN0 gastric cancer. Surg Today. 2016; 46:1031–1038. PMID: 26658717.
Article9. Toyokawa T, Ohira M, Tanaka H, Minamino H, Sakurai K, Nagami Y, et al. Optimal management for patients not meeting the inclusion criteria after endoscopic submucosal dissection for gastric cancer. Surg Endosc. 2016; 30:2404–2414. PMID: 26463497.
Article10. Suzuki H, Oda I, Abe S, Sekiguchi M, Mori G, Nonaka S, et al. High rate of 5-year survival among patients with early gastric cancer undergoing curative endoscopic submucosal dissection. Gastric Cancer. 2016; 19:198–205. PMID: 25616808.
Article11. Lee YJ, Jeong SH, Hur H, Han SU, Min JS, An JY, et al. Prospective multicenter feasibility study of laparoscopic sentinel basin dissection for organ preserving surgery in gastric cancer: quality control study for surgical standardization prior to phase III trial. Medicine (Baltimore). 2015; 94:e1894. PMID: 26512607.12. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009; 250:187–196. PMID: 19638912.13. Ryu KW, Eom BW, Nam BH, Lee JH, Kook MC, Choi IJ, et al. Is the sentinel node biopsy clinically applicable for limited lymphadenectomy and modified gastric resection in gastric cancer? A meta-analysis of feasibility studies. J Surg Oncol. 2011; 104:578–584. PMID: 21695700.
Article14. Arigami T, Uenosono Y, Yanagita S, Matsushita D, Arima H, Hirata M, et al. Feasibility of sentinel node navigation surgery after noncurative endoscopic resection for early gastric cancer. J Gastroenterol Hepatol. 2013; 28:1343–1347. PMID: 23663136.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Non-exposure Simple Suturing Endoscopic Full-thickness Resection with Sentinel Basin Dissection in Patients with Early Gastric Cancer: the SENORITA 3 Pilot Study
- Recent Advances in Sentinel Node Navigation Surgery for Early Gastric Cancer
- Laparoscopic Sentinel Node Navigation Surgery for Gastric Cancer
- Endoscopic Submucosal Dissection in the Treatment of Patients With Papillary Early Gastric Cancer
- Safety of Laparoscopic Sentinel Basin Dissection in Patients with Gastric Cancer: an Analysis from the SENORITA Prospective Multicenter Quality Control Trial
