Cup-Cage Construct Using Porous Cup with Burch-Schneider Cage in the Management of Complex Acetabular Fractures
- Affiliations
-
- 1Department of Orthopedics, All India Institute of Medical Sciences (AIIMS), New Delhi, India. cmcdeepak@yahoo.com
- KMID: 2448027
- DOI: http://doi.org/10.5371/hp.2019.31.2.87
Abstract
- PURPOSE
Cup-cage construct technique was developed to address the massive acetabular defects during revision hip arthroplasty. Indications have extended to complex acetabular fractures with pelvic discontinuity necessitating acute total hip arthroplasty. However, its use is constrained in low socioeconomic countries due to non-availability of the original cages from Trabecular Metal Acetabular Revision System and high cost. We used a novel technique using the less expensive Burch-Schneider (BS) cage and Trabecular Metal Revision Shell (TMRS) to address the problem.
MATERIALS AND METHODS
We reviewed a consecutive series of 8 cases of acetabular fractures reconstructed using a "˜cup-cage construct' technique using a BS cage along with a TMRS. The mean age of the patients was 61.4 years. Patients were followed up for a mean period of 50.5 months (24 to 72 months). The patients were assessed clinically with Harris Hip Score and radiologically with serial X-rays.
RESULTS
All the patients were available at the latest follow up. The mean Harris Hip Score was 87.2. There was no radiological evidence of failure. One patient had dislocation two months following the surgery, which was treated by closed reduction and hip abduction brace. One patient developed an infection at 3 weeks necessitating debridement. The same patient had sciatic nerve palsy that recovered after 4 months.
CONCLUSION
This novel technique of the cup-cage construct seems to provide a stable construct at short to midterm follow-up. However, a long-term follow up would be required.
MeSH Terms
Figure
-
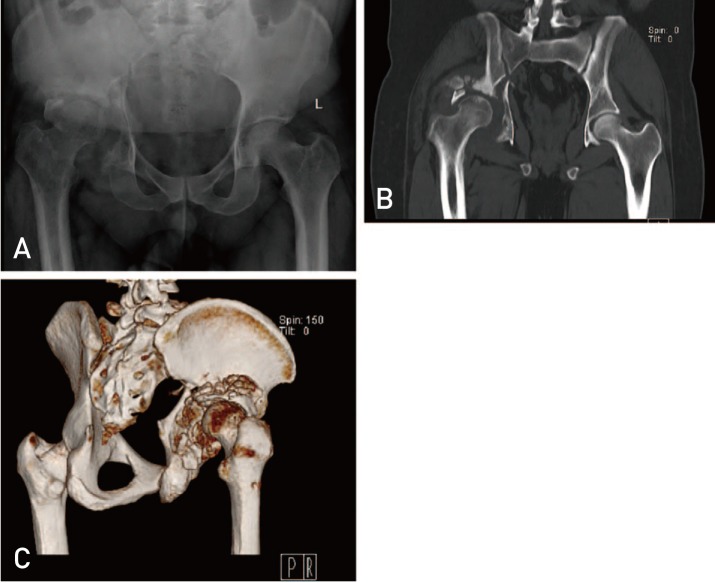
Fig. 1 (A) X-ray both hips with pelvis in anteroposterior view showing acetabular fracture in right side. (B) Computed tomogram scan of the pelvis in coronal section showing comminuted fracture of the acetabulum. Note the pelvic discontinuity. (C) Three-dimensional reconstruction computed tomogram showing the posterior aspect of the right hip. Note the comminuted fragments and near complete loss of bone in posterior column.

Fig. 2 Burch-Schneider cage.
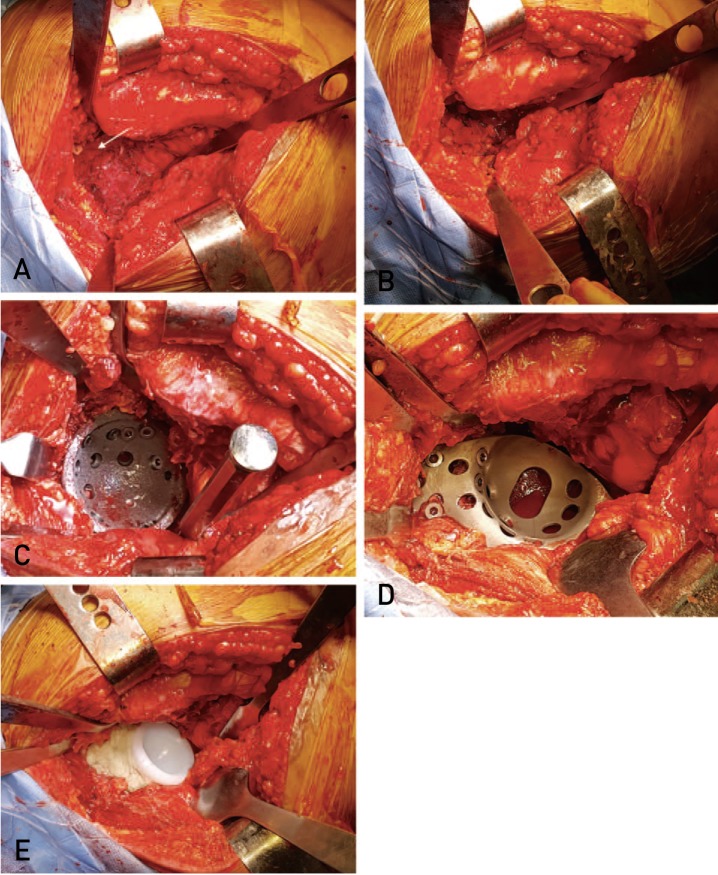
Fig. 3 (A) Exposure of the acetabulum. White arrow showing the only acetabular bone that was intact. Only soft tissue seen in the acetabular bed due to bone loss. (B) The acetabulum filled up with autografts from the resected femoral head. (C) Impaction of the trabecular metal shell and fixed with multiple screws. (D) Placement of the Burch-Schneider cage onto the acetabular shell and fixed with screws. The lower flange is into the osteotomy made in the ischium. (E) A polyethylene liner cemented onto the cage.
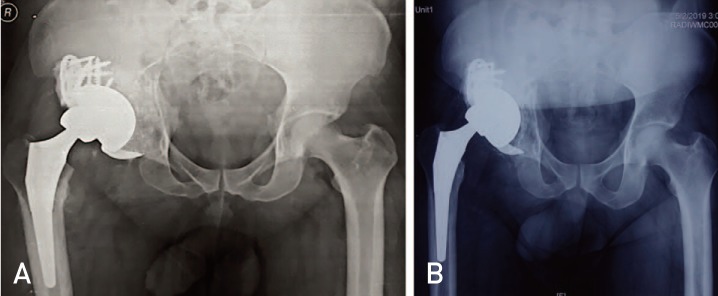
Fig. 4 4. (A) Immediate post-operative X-ray of the same patient (in Fig. 1 and 3) showing reconstructed right hip with cup-cage construct technique. (B) Four-year follow up X-ray of the same patient showing the cup-cage components in situ. The fracture has healed and the component position is unchanged as compared to the immediate post-operative X-ray.
Reference
-
1. Matta JM, Merritt PO. Displaced acetabular fractures. Clin Orthop Relat Res. 1988; (230):83–97.
Article2. Anglen JO, Burd TA, Hendricks KJ, Harrison P. The “Gull Sign”: a harbinger of failure for internal fixation of geriatric acetabular fractures. J Orthop Trauma. 2003; 17:625–634. PMID: 14574190.3. Bhandari M, Matta J, Ferguson T, Matthys G. Predictors of clinical and radiological outcome in patients with fractures of the acetabulum and concomitant posterior dislocation of the hip. J Bone Joint Surg Br. 2006; 88:1618–1624. PMID: 17159175.
Article4. Kreder HJ, Rozen N, Borkhoff CM, et al. Determinants of functional outcome after simple and complex acetabular fractures involving the posterior wall. J Bone Joint Surg Br. 2006; 88:776–782. PMID: 16720773.
Article5. Mears DC. Surgical treatment of acetabular fractures in elderly patients with osteoporotic bone. J Am Acad Orthop Surg. 1999; 7:128–141. PMID: 10217820.
Article6. Guerado E, Cano JR, Cruz E. Fractures of the acetabulum in elderly patients: an update. Injury. 2012; 43(Suppl 2):S33–S41. PMID: 23622990.
Article7. Sierra RJ, Mabry TM, Sems SA, Berry DJ. Acetabular fractures: the role of total hip replacement. Bone Joint J. 2013; 95-B(11 Suppl A):11–16. PMID: 24187344.8. De Bellis UG, Legnani C, Calori GM. Acute total hip replacement for acetabular fractures: a systematic review of the literature. Injury. 2014; 45:356–361. PMID: 24112700.
Article9. Mears DC, Velyvis JH. Acute total hip arthroplasty for selected displaced acetabular fractures: two to twelve-year results. J Bone Joint Surg Am. 2002; 84:1–9.10. Malhotra R, Singh DP, Jain V, Kumar V, Singh R. Acute total hip arthroplasty in acetabular fractures in the elderly using the Octopus System: mid term to long term follow-up. J Arthroplasty. 2013; 28:1005–1009. PMID: 23523497.11. Saterbak AM, Marsh JL, Turbett T, Brandser E. Acetabular fractures classification of Letournel and Judet--a systematic approach. Iowa Orthop J. 1995; 15:184–196. PMID: 7634031.12. Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969; 51:737–755. PMID: 5783851.13. Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr. Ectopic ossification following total hip replacement. Incidence and a method of classification. J Bone Joint Surg Am. 1973; 55:1629–1632. PMID: 4217797.14. Grubor P, Krupic F, Biscevic M, Grubor M. Controversies in treatment of acetabular fracture. Med Arch. 2015; 69:16–20. PMID: 25870470.
Article15. Zha GC, Sun JY, Dong SJ. Predictors of clinical outcomes after surgical treatment of displaced acetabular fractures in the elderly. J Orthop Res. 2013; 31:588–595. PMID: 23192663.
Article16. Moed BR, WillsonCarr SE, Watson JT. Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am. 2002; 84:752–758. PMID: 12004016.
Article17. Carpintero P, Caeiro JR, Carpintero R, Morales A, Silva S, Mesa M. Complications of hip fractures: a review. World J Orthop. 2014; 5:402–411. PMID: 25232517.
Article18. O'Toole RV, Hui E, Chandra A, Nascone JW. How often does open reduction and internal fixation of geriatric acetabular fractures lead to hip arthroplasty? J Orthop Trauma. 2014; 28:148–153. PMID: 23719343.19. Berry DJ. Antiprotrusio cages for acetabular revision. Clin Orthop Relat Res. 2004; (420):106–112.
Article20. Carroll FA, Hoad-Reddick DA, Kerry RM, Stockley I. The survival of support rings in complex acetabular revision surgery. J Bone Joint Surg Br. 2008; 90:574–578. PMID: 18450621.
Article21. Hipfl C, Janz V, Löchel J, Perka C, Wassilew GI. Cup-cage reconstruction for severe acetabular bone loss and pelvic discontinuity: mid-term results of a consecutive series of 35 cases. Bone Joint J. 2018; 100-B:1442–1448. PMID: 30418066.22. Hanssen AD, Lewallen DG. Modular acetabular augments: composite void fillers. Orthopedics. 2005; 28:971–972. PMID: 16190073.
Article23. Ballester Alfaro JJ, Sueiro Fernández J. Trabecular Metal buttress augment and the Trabecular Metal cup-cage construct in revision hip arthroplasty for severe acetabular bone loss and pelvic discontinuity. Hip Int. 2010; 20(Suppl 7):S119–S127. PMID: 20512783.
Article24. Kellet CF, Gross AE, Backstein D, Safir O. Massive acetabular bone loss: the cup-cage solution. Semin Arthroplast. 2010; 21:57–61.25. Kosashvili Y, Backstein D, Safir O, Lakstein D, Gross AE. Acetabular revision using an anti-protrusion (ilio-ischial) cage and trabecular metal acetabular component for severe acetabular bone loss associated with pelvic discontinuity. J Bone Joint Surg Br. 2009; 91:870–876. PMID: 19567849.
Article26. Abolghasemian M, Tangsaraporn S, Drexler M, et al. The challenge of pelvic discontinuity: cup-cage reconstruction does better than conventional cages in mid-term. Bone Joint J. 2014; 96-B:195–200. PMID: 24493184.27. Amenabar T, Rahman WA, Hetaimish BM, Kuzyk PR, Safir OA, Gross AE. Promising mid-term results with a cup-cage construct for large acetabular defects and pelvic discontinuity. Clin Orthop Relat Res. 2016; 474:408–414. PMID: 25712864.
Article28. Paprosky WG, O'Rourke M, Sporer SM. The treatment of acetabular bone defects with an associated pelvic discontinuity. Clin Orthop Relat Res. 2005; 441:216–220. PMID: 16331006.
Article29. Sporer SM, Paprosky WG. Acetabular revision using a trabecular metal acetabular component for severe acetabular bone loss associated with a pelvic discontinuity. J Arthroplasty. 2006; 21(6 Suppl 2):87–90. PMID: 16950068.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acetabular Cup Revision
- Management of Intraoperative Acetabular Fractures in Total Hip Arthroplasty: A Current Concept Review
- Bone Ingrowth Rate on Retrieved Human Porous-Coated Acetabular Cup
- A Clinical Study of Microporous Coated Hemispherical Acetabular Cup - A comparative Study in Relation to the Size of Acetabular Reaming-
- Total Hip Arthroplasty with Cemented Dual Mobility Cup into a Fully Porous Multihole Cup with Variable Angle Locking Screws for Acetabular Fractures in the Frail Elderly
