Development of the pulmonary pleura with special reference to the lung surface morphology: a study using human fetuses
- Affiliations
-
- 1Department of Anatomy, Tokyo Dental College, Tokyo, Japan. yamamotomasahito@tdc.ac.jp
- 2Institute of Anatomy and Cell Biology, School of Medicine, Georg-August-Universität Gőttingen, Gőttingen, Germany.
- 3Department of Anatomy, Akita University School of Medicine, Akita, Japan.
- 4Division of Internal Medicine, Iwamizawa Asuka Hospital, Iwamizawa, Japan.
- 5Department of Anatomy and Human Embryology, Institute of Embryology, Faculty of Medicine, Complutense University, Madrid, Spain.
- KMID: 2447007
- DOI: http://doi.org/10.5115/acb.2018.51.3.150
Abstract
- In and after the third trimester, the lung surface is likely to become smooth to facilitate respiratory movements. However, there are no detailed descriptions as to when and how the lung surface becomes regular. According to our observations of 33 fetuses at 9-16 weeks of gestation (crown-rump length [CRL], 39-125 mm), the lung surface, especially its lateral (costal) surface, was comparatively rough due to rapid branching and outward growing of bronchioli at the pseudoglandular phase of lung development. The pulmonary pleura was thin and, beneath the surface mesothelium, no or little mesenchymal tissue was detectable. Veins and lymphatic vessels reached the lung surface until 9 weeks and 16 weeks, respectively. In contrast, in 8 fetuses at 26-34 weeks of gestation (CRL, 210-290 mm), the lung surface was almost smooth because, instead of bronchioli, the developing alveoli faced the external surfaces of the lung. Moreover, the submesothelial tissue became thick due to large numbers of dilated veins connected to deep intersegmental veins. CD34-positive, multilayered fibrous tissue was also evident beneath the mesothelium in these stages. The submesothelial tissue was much thicker at the basal and mediastinal surfaces compared to apical and costal surfaces. Overall, rather than by a mechanical stress from the thoracic wall and diaphragm, a smooth lung surface seemed to be established largely by the thick submesothelial tissue including veins and lymphatic vessels until 26 weeks.
MeSH Terms
Figure
-
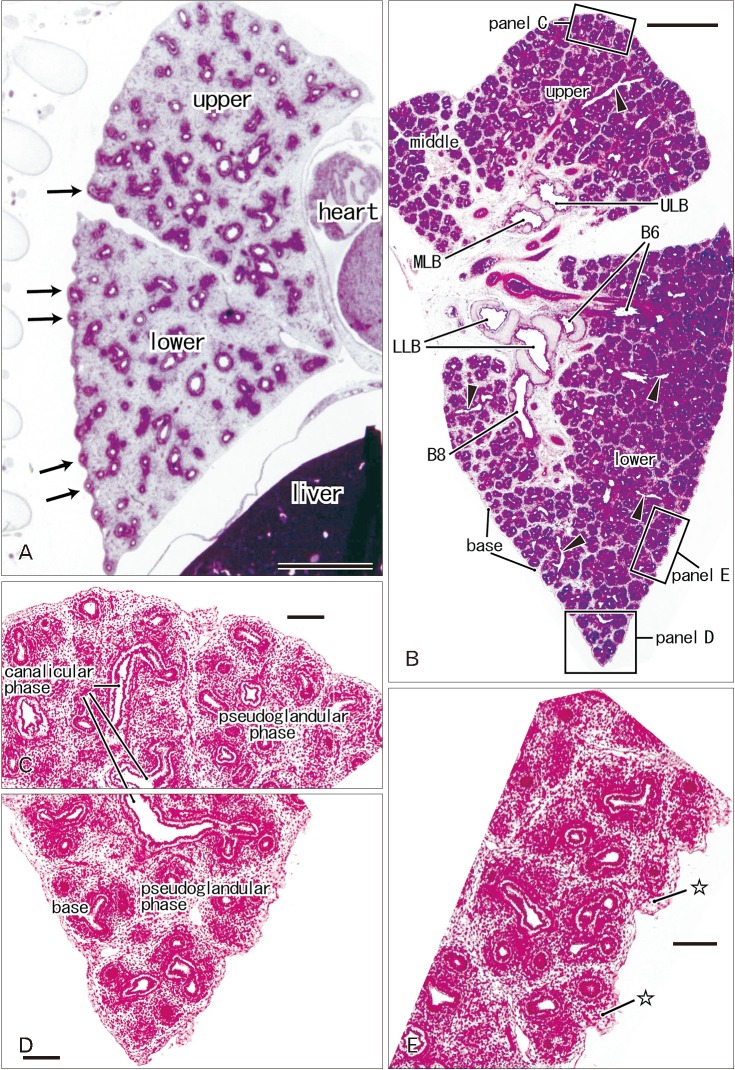
Fig. 1 Rough lung surface and pulmonary pleura at the pseudoglandular and canalicular phases. H&E staining. Sagittal sections. Panel A displays the left lung from a specimen at 9 weeks (39 mm crown-rump length [CRL]), while panels B–D exhibit the right lung from a specimen at 10 weeks (56 mm CRL). Panels C–E are higher magnification view of squares in panel B, respectively. In panel A, outward growing bronchi provide small protrusions of the lateral or costal surface (arrows). A rough surface is also evident in the costal aspect in panel B, but a mesenchymal tissue (stars) is present beneath the thin pleura (E). Deep intersegmental veins do not reach the lung surface (arrowheads in B). The canalicular phase of the bronchus was mixed with the pseudoglandular phase. upper, upper lobe; middle, middle lobe; lower, lower lobe; B6 and B8, sixth and eighth segmental bronchi; LLB, lower lobar bronchus; MLB, middle lobar bronchus; ULB, upper lobar bronchus. Scale bars=1 mm (A, B), 0.1 mm (C–E).
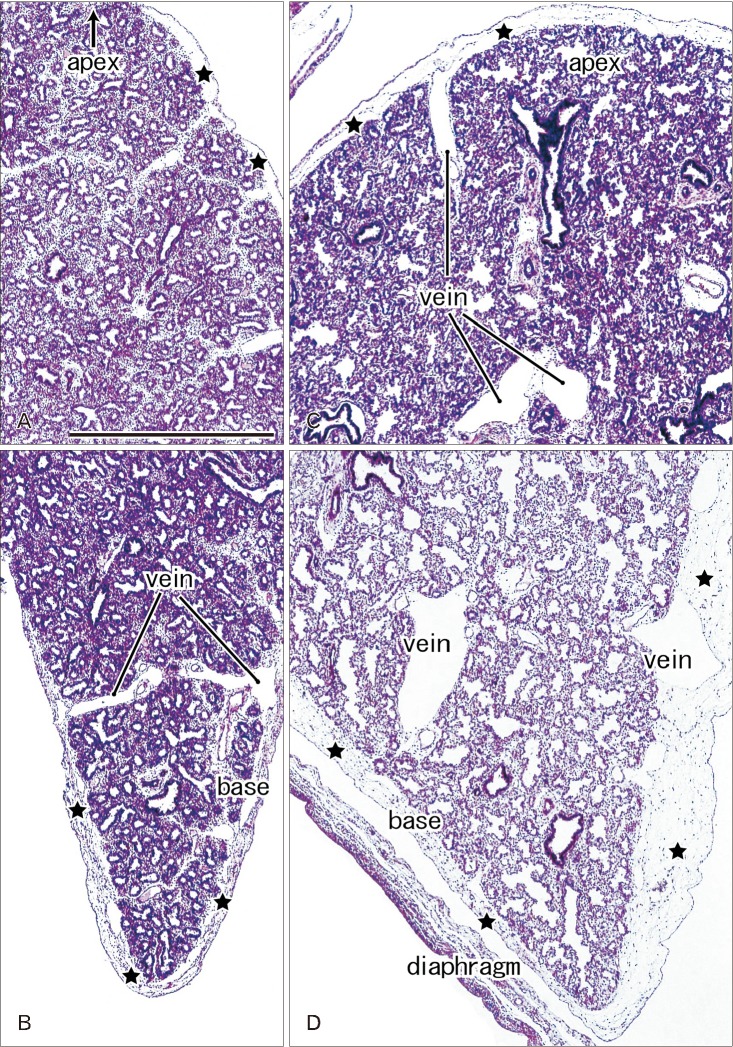
Fig. 2 Lung surface and pulmonary pleura at the saccular phase in late stage fetuses. H&E staining. Sagittal sections. Panels A and B display the left lung from a specimen at 26 weeks (215 mm crown-rump length [CRL]), while panels C and D exhibit the right lung from a specimen at 31 weeks (255 mm CRL). The subpleural tissue (stars) is thicker in the basal area than in the upper area near the apex of the lung and it contains dilated superficial veins those connected with deep, intersegmental veins. All panels were prepared at the same magnification. Scale bar=1 mm (A).
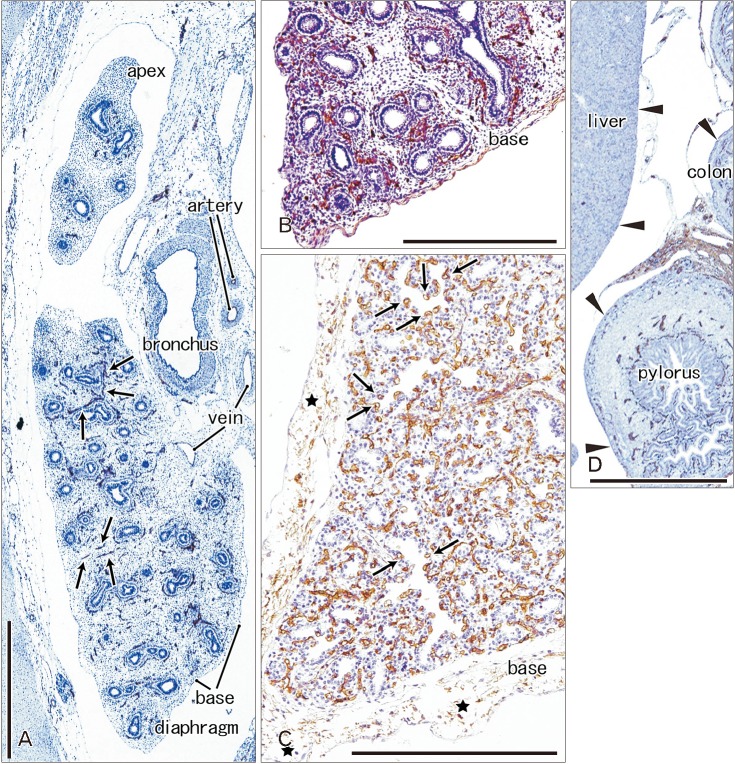
Fig. 3 CD34 immunohistochemistry of the lung and pleura. Sagittal sections. (A) The left lung from a specimen at 9 weeks (pseudoglandular phase; 39 mm crown-rump length [CRL]). (B) The left lung from a specimen at 15 weeks (a mixture of the pseudoglandular and canalicular phases; 115 mm CRL). (C) The left lung from a specimen at 30 weeks (saccular phase; 250 mm CRL). Panels B and D are photos of the same section and panel D displays the liver, pylorus and transverse colon. CD34 immunoreactivity is restricted in the developing vessels (arrows in A). At 15 weeks, the subpleural tissue is thin at the lung base (B), while no or little serosal tissue is seen along the liver, pylorus and colon (arrowheads in D). At 30 weeks, the subpleural tissue contains multilayered fibers expressing CD34 weakly (C). Capillaries adjacent to alveoli express CD34 strongly (arrows in C). Scale bars=1 mm.

Fig. 4 D2-40 immunohistochemistry of lymphatic vessels at the lung surface. (A) The right lung base from a specimen at 9 weeks (the same specimen as shown in Fig. 3A; 39 mm crown-rump length [CRL]). (B) The right lung base from a specimen at 16 weeks (a mixture of the pseudoglandular and canalicular phases; 125 mm CRL). D2-40–positive lymphatic vessels reach the lung surface until 9 weeks (arrows in A) and they are thick and abundant at 16 weeks (arrows in B). Bronchial epithelia also express reactivity of D2-40. Veins reach the lung surface at 16 weeks. Two panels were prepared at the same magnification. Scale bar=1 mm (A).

Fig. 5 Elastica Masson staining of the lung in late stage fetuses. Sagittal sections. Panels A and B display the left lung from a specimen at 26 weeks (215 mm crown-rump length [CRL]) and the right lung from a specimen at 31 weeks (255 mm CRL), respectively. Panel C exhibits a thick branch of the pulmonary artery from a specimen at 31 weeks (255 mm CRL). The pleura and subpleural tissue are stained dark gray (A, B), but they are different from wavy elastic fibers seen in the internal lamina of the arterial wall (C). All panels were prepared at the same magnification. Scale bar=0.1 mm (A).
Reference
-
1. Finley DJ, Rusch VW. Anatomy of the pleura. Thorac Surg Clin. 2011; 21:157–163. PMID: 21477764.2. O'Rahilly R, Müller F. Human embryology and teratology. 2nd ed. New York: Wiley-Liss;1996. p. 265–271.3. Hayashi S, Fukuzawa Y, Rodríguez-Vázquez JF, Cho BH, Verdugo-López S, Murakami G, Nakano T. Pleuroperitoneal canal closure and the fetal adrenal gland. Anat Rec (Hoboken). 2011; 294:633–644. PMID: 21370493.4. Abe S, Suzuki M, Cho KH, Murakami G, Cho BH, Ide Y. CD34-positive developing vessels and other structures in human fetuses: an immunohistochemical study. Surg Radiol Anat. 2011; 33:919–927. PMID: 21789504.5. Katori Y, Kiyokawa H, Kawase T, Murakami G, Cho BH. CD34-positive primitive vessels and other structures in human fetuses: an immunohistochemical study. Acta Otolaryngol. 2011; 131:1086–1090. PMID: 21651317.6. Wilting J, Papoutsi M, Christ B, Nicolaides KH, von Kaisenberg CS, Borges J, Stark GB, Alitalo K, Tomarev SI, Niemeyer C, Rössler J. The transcription factor Prox1 is a marker for lymphatic endothelial cells in normal and diseased human tissues. FASEB J. 2002; 16:1271–1273. PMID: 12060670.7. Hasselhof V, Sperling A, Buttler K, Ströbel P, Becker J, Aung T, Felmerer G, Wilting J. Morphological and molecular characterization of human dermal lymphatic collectors. PLoS One. 2016; 11:e0164964. PMID: 27764183.8. Kinoshita H, Umezawa T, Omine Y, Kasahara M, Rodríguez-Vázquez JF, Murakami G, Abe S. Distribution of elastic fibers in the head and neck: a histological study using late-stage human fetuses. Anat Cell Biol. 2013; 46:39–48. PMID: 23560235.9. Motohashi O, Suzuki M, Shida N, Umezawa K, Ohtoh T, Sakurai Y, Yoshimoto T. Subarachnoid haemorrhage induced proliferation of leptomeningeal cells and deposition of extracellular matrices in the arachnoid granulations and subarachnoid space. Immunhistochemicalstudy. Acta Neurochir (Wien). 1995; 136:88–91. PMID: 8748833.10. Hayashi T, Kumasaka T, Mitani K, Yao T, Suda K, Seyama K. Loss of heterozygosity on tuberous sclerosis complex genes in multifocal micronodular pneumocyte hyperplasia. Mod Pathol. 2010; 23:1251–1260. PMID: 20526286.11. Riquet M. Anatomic basis of lymphatic spread from carcinoma of the lung to the mediastinum: surgical and prognostic implications. Surg Radiol Anat. 1993; 15:271–277. PMID: 8128334.12. Topol M, Masłoń A. The problem of direct lymph drainage of the bronchopulmonary segments into the mediastinal and hilar lymph nodes. Clin Anat. 2009; 22:509–516. PMID: 19306320.13. Skandalakis JE, Gray SW, Symbas PN. The trachea and lungs. In : Skandalakis JE, Gray SW, editors. Embryology for Surgeons. 2nd ed. Baltimore, MD: Williams & Wilkins;1972. p. 414–450.14. Virtanen I, Laitinen A, Tani T, Pääkkö P, Laitinen LA, Burgeson RE, Lehto VP. Differential expression of laminins and their integrin receptors in developing and adult human lung. Am J Respir Cell Mol Biol. 1996; 15:184–196. PMID: 8703474.15. Arai H, Hirano H, Mushiake S, Nakayama M, Takada G, Sekiguchi K. Loss of EDB+ fibronectin isoform is associated with differentiation of alveolar epithelial cells in human fetal lung. Am J Pathol. 1997; 151:403–412. PMID: 9250153.16. Wright C, Strauss S, Toole K, Burt AD, Robson SC. Composition of the pulmonary interstitium during normal development of the human fetus. Pediatr Dev Pathol. 1999; 2:424–431. PMID: 10441619.17. Lambropoulou M, Limberis V, Koutlaki N, Simopoulou M, Ntanovasilis D, Vandoros GP, Tatsidou P, Kekou I, Koutsikogianni I, Papadopoulos N. Differential expression of tenascin-C in the developing human lung: an immunohistochemical study. Clin Exp Med. 2009; 9:333–338. PMID: 19626416.18. Jin ZW, Nakamura T, Yu HC, Kimura W, Murakami G, Cho BH. Fetal anatomy of peripheral lymphatic vessels: a D2-40 immunohistochemical study using an 18-week human fetus (CRL 155 mm). J Anat. 2010; 216:671–682. PMID: 20408907.19. Kim JH, Han EH, Jin ZW, Lee HK, Fujimiya M, Murakami G, Cho BH. Fetal topographical anatomy of the upper abdominal lymphatics: its specific features in comparison with other abdominopelvic regions. Anat Rec (Hoboken). 2012; 295:91–104. PMID: 22144396.
