Kosin Med J.
2018 Dec;33(3):391-395. 10.7180/kmj.2018.33.3.391.
Case Report of Prostate Cancer Patient with Only Lymph Node Involvement on F-18 FDG PET/CT
- Affiliations
-
- 1Department of Urology, School of Medicine, Catholic University of Daegu, Korea.
- 2Department of Nuclear Medicine School of Medicine, Catholic University of Daegu, Korea. kufa77@hanmail.net
- KMID: 2442550
- DOI: http://doi.org/10.7180/kmj.2018.33.3.391
Abstract
- We report a case of a patient with locally advanced prostate cancer who had only lymph node involvement without bone metastasis on F-18 FDG PET/CT. A 62-year-old Korean male was admitted to our hospital due to dysuria. His PSA level on admission was 79.35 ng/mL. A transrectal ultrasound-guided prostate biopsy confirmed prostate cancer and his Gleason score was 10 (5+5). F-18 FDG PET/CT demonstrated a hypermetabolic mass lesion with SUVmax 7.0 in the prostate and hypermetabolism with SUVmax 4.7 of the abdominal and pelvic lymph nodes. Tc-99m HDP bone scan showed no significant bone metastasis. The patient underwent hormonal therapy for 9 months. Follow-up F-18 FDG PET/CT showed significantly reduced size and FDG uptake in the prostate and abdominal and pelvic lymph nodes. In this case, treatment monitoring with F-18 FDG PET/CT showed decreased mass size and FDG uptake in the prostate and abdominal and pelvic lymph nodes.
MeSH Terms
Figure
-
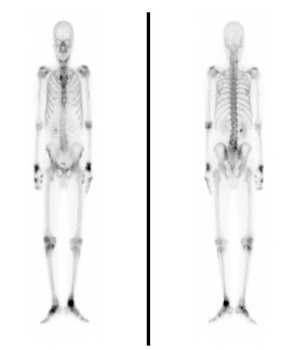
Fig. 1 A 62-year-old male underwent Tc-99m HDP bone scintigraphy for searching bone metastasis. Tc-99m HDP bone scintigraphy showed multiple tracer uptake in the wrist, knee, ankle and hand joints, associated with arthritis, but no significant focal tracer uptake of bone metastasis.
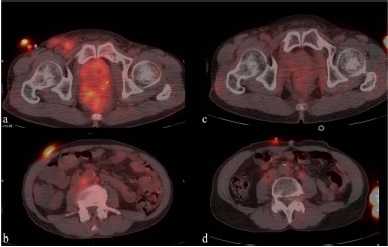
Fig. 2 F-18 FDG PET/CT showed a mass lesion with FDG uptake with SUVmax 4.6 in the prostate (a) and lymph node enlargement with FDG uptake with SUVmax 3.4 in paraaortic (b) areas. Follow-up F-18 FDG PET/CT about 9 months after hormonal therapy showed a significantly reduced size and FDG uptake in the prost
Reference
-
1. Scher HI, Halabi S, Tannock I, Morris M, Sternberg CN, Carducci MA, et al. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol. 2008; 26:1148–1159.
Article2. Basu S, Alavi A. Unparalleled contribution of 18F-FDG PET to medicine over 3 decades. J Nucl Med. 2008; 49:17N–21N. 37N3. Gambhir SS. Molecular imaging of cancer with positron emission tomography. Nat Rev Cancer. 2002; 2:683–693.
Article4. Phelps ME. PET: the merging of biology and imaging into molecular imaging. J Nucl Med. 2000; 41:661–681.5. Jadvar H. FDG PET in Prostate Cancer. PET clinics. 2009; 4:155–161.
Article6. Lebret T, Mejean A. [Rare locations of metastases from prostate cancer]. Prog Urol. 2008; 18:S357–S364.7. Venara A, Thibaudeau E, Lebdai S, Mucci S, Ridereau-Zins C, Azzouzi R, et al. Rectal metastasis of prostate cancer: about a case. J Clin med res. 2010; 2:137–139.
Article8. Bowrey DJ, Otter MI, Billings PJ. Rectal infiltration by prostatic adenocarcinoma: report on six patients and review of the literature. Ann R Coll Surg Engl. 2003; 85:382–385.
Article9. Liu L, Devine P, Einhorn E, Kao GD. Incidental finding of an isolated prostate cancer metastasis in an inguinal hernial sac. J Urol. 2000; 164:457–458.
Article10. Kanamaru H, Oyama N, Akino H, Okada K. [Evaluation of prostate cancer using FDG-PET]. Hinyokika kiyo. 2000; 46:851–853.11. Liu IJ, Zafar MB, Lai YH, Segall GM, Terris MK. Fluorodeoxyglucose positron emission tomography studies in diagnosis and staging of clinically organ-confined prostate cancer. Urology. 2001; 57:108–111.
Article12. Jadvar H, Pinski JK, Conti PS. FDG PET in suspected recurrent and metastatic prostate cancer. Oncology reports. 2003; 10:1485–1488.
Article13. Agus DB, Golde DW, Sgouros G, Ballangrud A, Cordon-Cardo C, Scher HI. Positron emission tomography of a human prostate cancer xenograft: association of changes in deoxyglucose accumulation with other measures of outcome following androgen withdrawal. Cancer Res. 1998; 58:3009–3014.14. Oyama N, Akino H, Suzuki Y, Kanamaru H, Sadato N, Yonekura Y, et al. The increased accumulation of [18F]fluorodeoxyglucose in untreated prostate cancer. Jpn J Clin Oncol. 1999; 29:623–629.
Article15. Sanz G, Robles JE, Gimenez M, Arocena J, Sánchez D, Rodriguez-Rubio F, et al. Positron emission tomography with 18fluorine-labelled deoxyglucose: utility in localized and advanced prostate cancer. BJU Int. 1999; 84:1028–1031.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- (18)F-FDG PET/CT with Contrast Enhancement for Evaluation of Axillary Lymph Node Involvement in T1 Breast Cancer
- Discrepancy of Bone Metastases between F-18 FDG PET/CT and Bone Scan in a Patient with Prostate Cancer
- Discordant Molecular Imaging Findings with 2‑[18F]FDG and [68Ga] Ga‑PSMA PET/CT in a Patient with Both Bladder and Prostate Cancer
- Comparison of Neck CT and ¹â¸F-FDG PET-CT for Making the Preoperative Diagnosis of Lymph Node Metastasis in Papillary Thyroid Cancer
- Unusual Contralateral Axillary Lymph Node Metastasis in a Second Primary Breast Cancer Detected by FDG PET/CT and Lymphoscintigraphy
