Comparison of the Outcomes of Two- and Three-muscle Surgery in Exotropia over 45 Prism Diopters
- Affiliations
-
- 1Department of Ophthalmology, Konkuk University School of Medicine, Seoul, Korea. shineye@kuh.ac.kr
- KMID: 2440455
- DOI: http://doi.org/10.3341/jkos.2019.60.3.268
Abstract
- PURPOSE
We report the outcomes of two- or three-muscle surgery on patients with large-angle exotropia exceeding 45 prism diopters (PDs).
METHODS
We retrospectively analyzed data on 45 exotropia patients (> 45 PDs) who underwent two- or three-muscle surgery. We excluded patients with paralytic or restrictive strabismus, A- or V-pattern strabismus, a coexistent oblique dysfunction or nystagmus, and/or a history of prior extraocular muscle surgery. Only patients for whom at least 6 months of follow-up data were available were included. Successful surgery was defined as postoperative esotropia ≤ 5 PD, orthophoria, and exotropia ≤ 10 PD at the last visit.
RESULTS
We included 45 patients, of whom 22 and 23 underwent two- and three-muscle surgery, respectively. The mean postoperative deviations were 9.5 and 2.7 PD in the two- and three-muscle groups, respectively; the overall success rates were 54.55% (12/22) and 91.30% (21/23). Subgroup analyses revealed that the surgical success rate of two-muscle operations was 66.67% (12/18) in 45-55 PD patients and 0% (0/4) in ≥ 55 PD patients; the success rates of three-muscle operations were 100% (7/7) and 87.50% (14/16). The success rate did not differ significantly between those with postoperative deviations of 45-55 PD (p = 0.137), but did between those who underwent two- and three-muscle operations to treat postoperative deviations of ≥ 55 PD (p = 0.003).
CONCLUSIONS
Satisfactory results can be achieved via two-muscle surgery in patients with exotropia < 55 PD. However, for those with exotropia > 55 PD, three-muscle surgery is superior to two-muscle surgery. Therefore, large-angle exotropia is optimally treated via three-muscle surgery.
Figure
-

Figure 1 The duration of follow up as measured by the survival analysis (*Kaplan-Meier method). The mean duration of success of the two muscle group and the three muscle group was 86.59 ± 11.94 months and 124.65 ± 5.70 months, respectively.
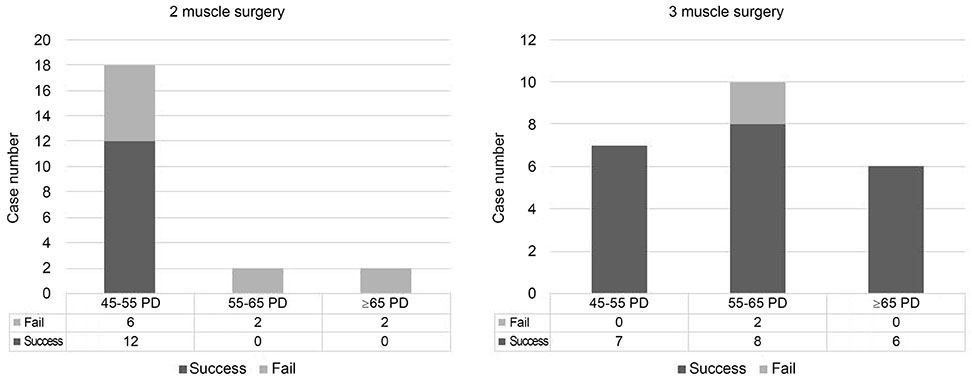
Figure 2 Success case according to the preoperative angle of deviation. The overall success rates were 63.6% (12/22) in two muscle groups and 91.3% (21/23) in three muscle groups. PD = prism diopters.
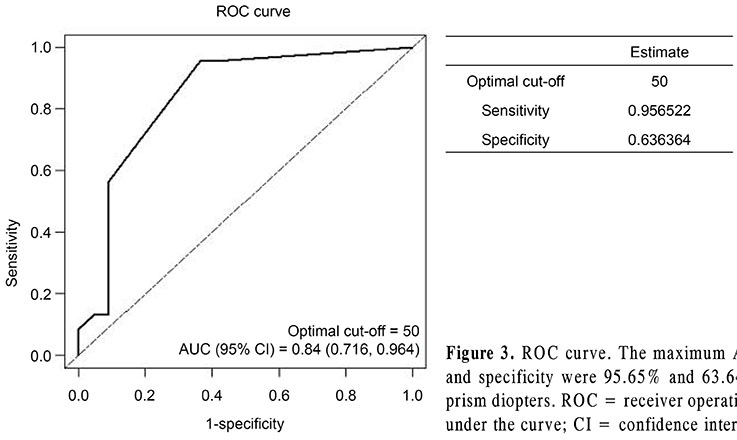
Figure 3 ROC curve. The maximum AUC is 0.84 and the sensitivity and specificity were 95.65% and 63.64% using a cut-off value of 50 prism diopters. ROC = receiver operating characteristics; AUC = area under the curve; CI = confidence interval.
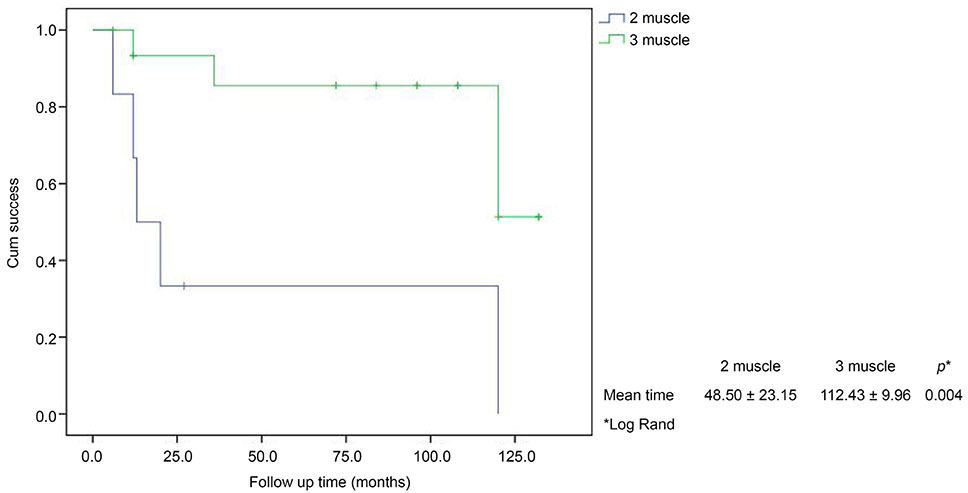
Figure 4 The duration of follow up as measured by the survival analysis (*Kaplan-Meier method) in 50–65 prism diopters exotropia. The mean duration of success in the two muscle group and the three muscle group was 48.50 ± 23.15 months and 112.43 ± 9.96 months, respectively.
Reference
-
1. Choi JW, Lee SG. Surgical outcomes of large-angle exotropia. J Korean Ophthalmol Soc. 2011; 52:959–963.
Article2. Hwang SW, Chang BL. The surgical outcome of bilateral lateral rectus recession in large angle exotropia. J Korean Ophthalmol Soc. 2000; 41:973–984.3. Shin DB, Song YJ, Lee SB, et al. Effect of both lateral rectus recession in large angle exotropia. J Korean Ophthalmol Soc. 2003; 44:1363–1369.4. Lim HS, Seo SW, Lee JH. Comparison of surgical results between bilateral rectus muscle recession and lateral rectus muscle recession and medial rectus muscle resection in exotropia over 40 prism diopters. J Korean Ophthalmol Soc. 1998; 39:2810–2815.5. Im SK, Park SW, Park YG. Effects of bilateral lateral rectus recession and unilateral recession-resection in large angle exotropia. J Korean Ophthalmol Soc. 2004; 45:990–994.6. Li JH, Zhang LJ. Three-muscle surgery for very large-angle constant exotropia. J AAPOS. 2013; 17:578–581.
Article7. Lau FH, Fan DS, Yip WW, et al. Surgical outcome of single-staged three horizontal muscles squint muscle surgery for extra-large angle exotropia. Eye (Lond). 2010; 24:1171–1176.8. Kim JW, Rah SH, Lee JH. The surgical treatment of exotropias of 60 prism diopters or more. J Korean Ophthalmol Soc. 1997; 38:2200–2206.9. Yang M, Chen J, Shen T, et al. Single stage surgical outcomes for large angle intermittent exotropia. PLoS One. 2016; 11:e0150508.
Article10. Mulberger RD, Mcdornald PR. Surgical management of nonparalytic exotropia. AMA Arch Ophthalmol. 1954; 52:664–668.
Article11. Schwartz RL, Calhoun JH. Surgery of large angle exotropia. J Pediatr Ophthalmol Strabismus. 1980; 17:359–363.
Article12. Park YG, Min BM. The effects of bilateral recti recessions over 8mm in exotropia over 40 prism diopters. J Korean Ophthalmol Soc. 1994; 35:1123–1126.13. Jampolsky A. Surgical management of exotropia. Am J Ophthalmol. 1958; 46(5 Part 1):646–648.
Article14. Taylor DM. How early is early surgery in management of strabismus. Arch Ophthalmol. 1963; 70:752–756.15. Thompson JT, Guyton DL. Ophthalmic prisms. Measurement errors and how to minimize them. Ophthalmology. 1983; 90:204–210.16. Wright KW, Strube YN. Color atlas of ophthalmic surgery strabismus. Philadelphia: JB Lippincott company;1991. p. 241–243.17. Gezer A, Sezen F, Nasri N, Gözüm N. Factors influencing the outcome of strabismus surgery in patient with exotropia. J AAPOS. 2004; 8:56–60.18. Scott AB, Marsh AJ, Jampolsky A. Quantitative guidelines for exotropia surgery. Invest Ophthalmol. 1975; 14:428–436.19. Guibor G. The surgical treatment of exotropia resulting from anterior internuclear ophthalmoplegia. A practical evaluation of some surgical techniques. Am J Ophthalmol. 1950; 33:1837–1842.20. Burke RM. Principle, technique and complications of horizontal nonparalytic nonaccomodative strabismus surgery. In : Haik GM, editor. Strabismus symphosium of the new orleans academy of ophthalmology. 1st ed. St. Louis: Mosby Co.;1962. p. 178–189.21. Chen JH, Morrison DG, Donahue SP. Three and four horizontal muscle surgery for large angle exotropia. J Pediatr Ophthalmol Strabismus. 2015; 52:305–310.
Article22. Burian HM, Spivey BE. The surgical management of exodeviations. Am J ophthalmol. 1965; 59:603–620.23. Urist MJ. Exotropia with bilateral elevation in adduction, II. Surgery. Am J Ophthalmol. 1954; 38:178–190.24. Berland JE, Wilson ME, Saunders RB. Results of large (8-9 mm) bilateral lateral rectus muscle recessions for exotropia. Binocul Vis Strabismus Q. 1998; 13:97–104.25. Brooks DR, Morrison DG, Donahue SP. The efficacy of superior oblique Z-tenotomy in the treatment of overdepression in adduction (superior oblique overaction). J AAPOS. 2012; 16:342–344.
Article26. Livir-Rallatos G, Gunton KB, Calhoun JH. Surgical results in large-angle exotropia. J AAPOS. 2002; 6:77–80.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgery in a Patient with Sensory Exotropia with an Abnormally Attached Lateral Rectus Muscle
- Outcomes of Augmented Surgery Performed after Simplified Prism Adaptation Testing in Patients with Intermittent Exotropia
- The Accuracy of Estimating Postoperative Deviation in Exotropia With over 40 Prism Diopters
- The Effect of Anterior Transposition of the Inferior Oblique Muscle with Marginal Myectomy in a Case of Lost Inferior Rectus Muscle
- The Effect of Occlusion Therapy on Overcorrected Monocular Exotropia
