Common Sites, Etiology, and Solutions of Persistent Septal Deviation in Revision Septoplasty
- Affiliations
-
- 1Dr. Jin's Premium Nose Clinic, Seoul, Korea.
- 2Department of Otorhinolaryngology-Head and Neck Surgery, SMG-SNU Boramae Medical Center, Seoul, Korea.
- 3Department of Otorhinolaryngology-Head and Neck Surgery, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju, Korea. hahnjin2@naver.com
- KMID: 2439856
- DOI: http://doi.org/10.21053/ceo.2017.01788
Abstract
OBJECTIVES
To investigate the common causes of persistent septal deviation in revision septoplasty and to report the surgical techniques and results to correct them.
METHODS
A total of 100 consecutive patients (86 males) who had revision septoplasty due to persistent septal deviation from 2008 and 2014 were included in the study. Their mean age was 35.6 years and the mean follow-up duration was 9.1 months. Presenting symptoms, sites of persistent septal deviation, techniques used to correct the deviation, and surgical results were reviewed.
RESULTS
The mean interval between primary and revision surgery was 6.2 years. Forty-eight patients received revision septoplasty and 52 received revision septoplasty combined with rhinoplasty. Nasal obstruction was the most presenting symptom in almost all patients. The most common site of persistent septal deviation was middle septum (58%) followed by caudal septum (31%). Correcting techniques included further chondrotomy and excision of deviated portion in 76% and caudal batten graft in 39%. Rhinoscopic and endoscopic exams showed straight septum in 97% and 92 patients had subjective symptom improvement postoperatively.
CONCLUSION
Middle septum and caudal septum were common sites of persistent deviation. Proper chondrotomy with excision of deviated middle septum and correction of the caudal deviation with batten graft are key maneuvers to treat persistent deviation.
Figure
-
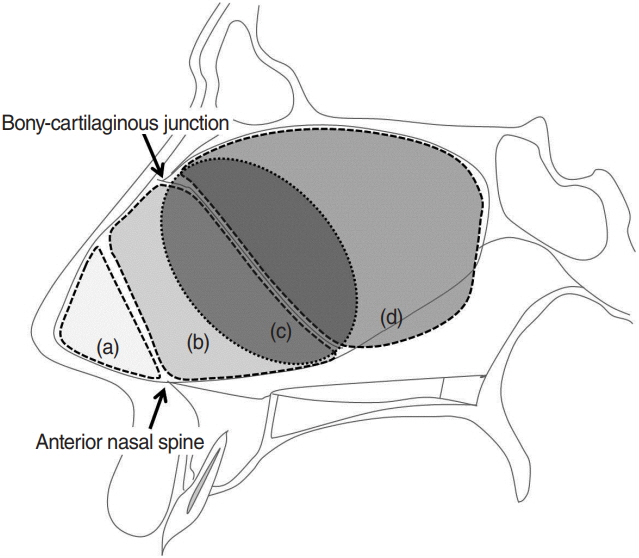
Fig. 1. Dividing the septum into four areas. a: Caudal septum (caudal end of cartilaginous septum), b: anterior septum (cartilaginous septum except caudal septum), c: middle septum (area around the bony-cartilaginous septum), d: posterior septum (bony septum).
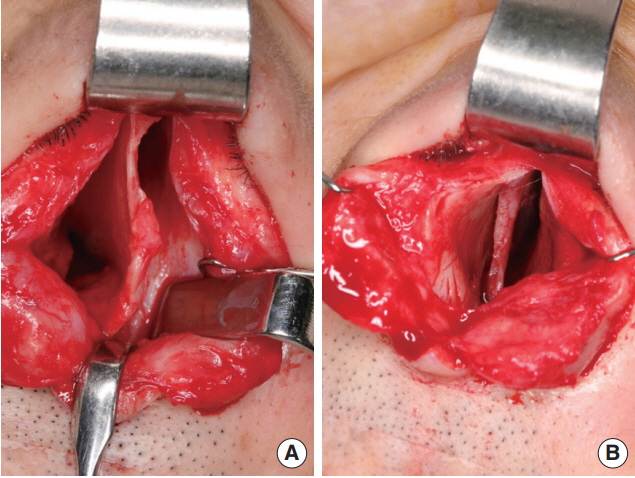
Fig. 2. Persistent curved deformity after septoplasty and more chondrotomy to relieve deforming forces of the bony septum. (A) Persistent curvature of the septal cartilage is observed after full exposure of the septum after separation from the upper lateral cartilages. (B) Further chondrotomy was done for correction. Partial hatching incision attempted at previous surgery is also observed at the inferior portion of the caudal septum.
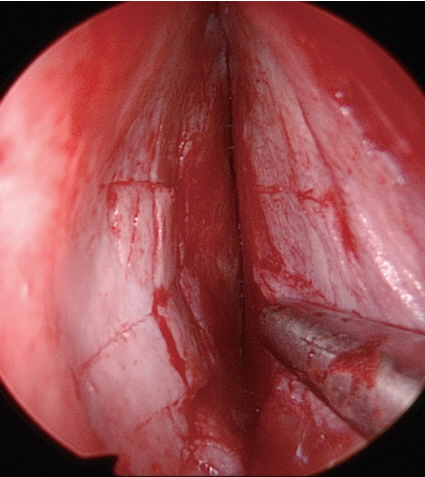
Fig. 3. Cross-hatching incisions performed on the concave side of septal cartilage at previous surgery are observed. Some of the incisions were too deep and some of them were too superficial and failed to correct the curvature of the septal cartilage.
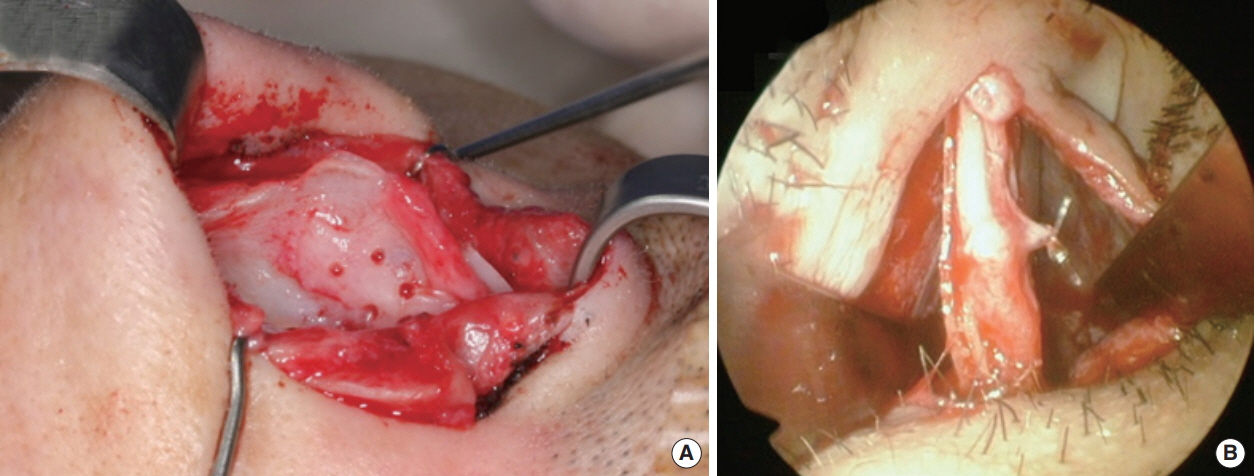
Fig. 4. Batten graft with septal bone to correct caudal septal deformity. (A) Open approach. (B) Endonasal approach.
Cited by 3 articles
-
Crosshatching Incision in Septoplasty: Abandoning an Old Myth
Hong Ryul Jin, Jong-Sook Yi
Clin Exp Otorhinolaryngol. 2020;13(1):4-5. doi: 10.21053/ceo.2019.01767.Evaluation of the Esthetic and Functional Outcomes of Extracorporeal Septoplasty for Rhinoplasty in Asian Patients
Sue Jean Mun, Young-Seok Choi, Ji Hwan Kim, Woo Sub Shim, Hahn Jin Jung
Clin Exp Otorhinolaryngol. 2021;14(1):100-107. doi: 10.21053/ceo.2019.01704.Caudal Septoplasty: A Useful Cartilage Stump on Anterior Nasal Spine
Myung Ho Jin, Myoung Su Choi
Korean J Otorhinolaryngol-Head Neck Surg. 2022;65(4):242-246. doi: 10.3342/kjorl-hns.2022.00045.
Reference
-
1. Uppal S, Mistry H, Nadig S, Back G, Coatesworth A. Evaluation of patient benefit from nasal septal surgery for nasal obstruction. Auris Nasus Larynx. 2005; Jun. 32(2):129–37.
Article2. Gillman GS, Egloff AM, Rivera-Serrano CM. Revision septoplasty: a prospective disease-specific outcome study. Laryngoscope. 2014; Jun. 124(6):1290–5.
Article3. Siegel NS, Gliklich RE, Taghizadeh F, Chang Y. Outcomes of septoplasty. Otolaryngol Head Neck Surg. 2000; Feb. 122(2):228–32.
Article4. Illum P. Septoplasty and compensatory inferior turbinate hypertrophy: long-term results after randomized turbinoplasty. Eur Arch Otorhinolaryngol. 1997; Jan. 254 Suppl 1:S89–92.
Article5. Fjermedal O, Saunte C, Pedersen S. Septoplasty and/or submucous resection? 5 Years nasal septum operations. J Laryngol Otol. 1988; Sep. 102(9):796–8.6. Lee BJ, Chung YS, Jang YJ. Overcorrected septum as a complication of septoplasty. Am J Rhinol. 2004; Nov-Dec. 18(6):393–6.
Article7. Becker SS, Dobratz EJ, Stowell N, Barker D, Park SS. Revision septoplasty: review of sources of persistent nasal obstruction. Am J Rhinol. 2008; Jul-Aug. 22(4):440–4.
Article8. Dinis PB, Haider H. Septoplasty: long-term evaluation of results. Am J Otolaryngol. 2002; Mar-Apr. 23(2):85–90.
Article9. Sedwick JD, Lopez AB, Gajewski BJ, Simons RL. Caudal septoplasty for treatment of septal deviation: aesthetic and functional correction of the nasal base. Arch Facial Plast Surg. 2005; May-Jun. 7(3):158–62.10. Murakami WT, Wong LW, Davidson TM. Applications of the biomechanical behavior of cartilage to nasal septoplastic surgery. Laryngoscope. 1982; Mar. 92(3):300–9.
Article11. Heo SJ, Kim JS. Crosshatching incision technique in septoplasty: experimental outcomes under actual surgical settings. Auris Nasus Larynx. 2016; Oct. 43(5):518–23.
Article12. Ozyazgan I, Idaci O. A new method that uses cyanoacrylate tissue adhesive to fill scoring incisions in septal cartilage correction. Laryngoscope. 2011; Jun. 121(6):1164–72.13. Min YG, Chung JW. Cartilaginous incisions in septoplasty. ORL J Otorhinolaryngol Relat Spec. 1996; Jan-Feb. 58(1):51–4.
Article14. Wee JH, Lee JE, Cho SW, Jin HR. Septal batten graft to correct cartilaginous deformities in endonasal septoplasty. Arch Otolaryngol Head Neck Surg. 2012; May. 138(5):457–61.
Article15. Chung YS, Seol JH, Choi JM, Shin DH, Kim YW, Cho JH, et al. How to resolve the caudal septal deviation? Clinical outcomes after septoplasty with bony batten grafting. Laryngoscope. 2014; Aug. 124(8):1771–6.
Article16. Haack J, Papel ID. Caudal septal deviation. Otolaryngol Clin North Am. 2009; Jun. 42(3):427–36.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Revision and Reconstructive Septoplasty
- Selection of Surgical Technique and Treatment Outcome of Revision Septoplasty
- The Effect of Nasal Septal Deviation and Septoplasty on Dacryocystorhinostomy Progression
- Correction of Caudal Septal Deviation: Septal Batten Graft with a Bioabsorbable Plate
- Septal deviation correction methods and surgical considerations in turbinoplasty
