Preganglionic Epidural Steroid Injection through Translateral Recess Approach
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul Red Cross Hospital, Seoul, Korea. orthopedicspinae@gmail.com
- 2Department of Orthopedic Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- KMID: 2438344
- DOI: http://doi.org/10.4055/cios.2019.11.1.131
Abstract
- The approach we suggest was developed for cases in which the fourth and fifth lumbar and first sacral spinal nerves were affected in lumbar degenerative disc disease. Retrodiscal transforaminal epidural injection is known to be very effective for lumbar radiculopathy because of excellent access to primary pathology; however, access below L5 is often restricted by the anatomic characteristics of the L5-S1. In the translateral recess approach (TLR), proper final needle placement (i.e., in the axillary portion between the exiting and traversing nerve roots) can be achieved by setting the direction of the needle laterally and superiorly from the distal tip of the infra-adjacent spinous process toward the medial wall of the pedicle and neural foramen of the given level without neural injury. This approach is possible because of the wide interlaminar space in the L5-S1. Preganglionic epidural injection through TLR is an effective and safe spinal intervention for lumbosacral radiculopathy.
Figure
-
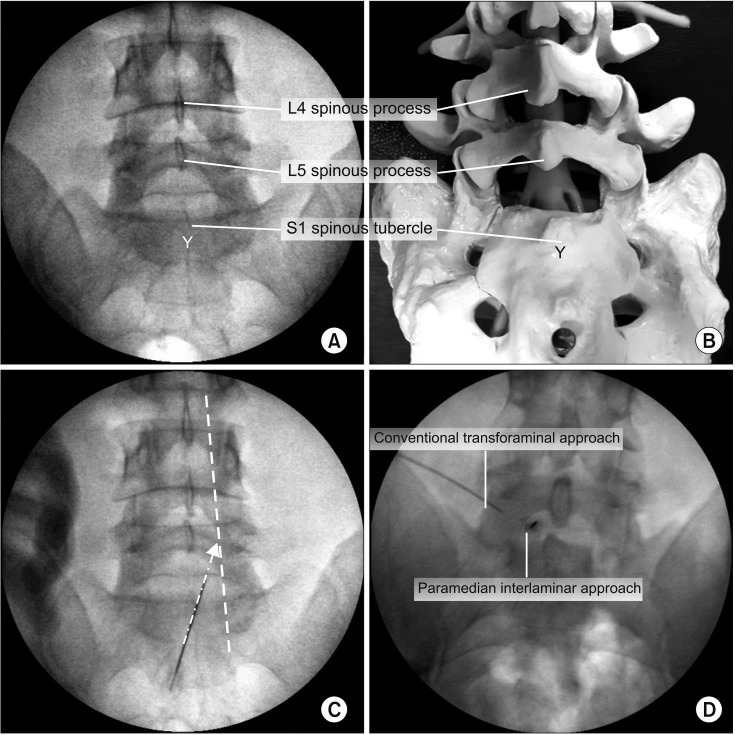
Fig. 1 Entry points of preganglionic epidural injection through translateral recess approach. (A) Distal portion of the S1 spinous tubercle has a “Y” shape in the lumbosacral standard anteroposterior (AP) image. Under fluoroscopic guidance, a 20G 3.5-inch Tuohy needle was inserted into the distal tip of the S1 spinous tubercle. (B) AP image of an artificial lumbar spine model. (C) Under fluoroscopic guidance, a 20G 3.5-inch Tuohy needle was advanced toward the medial wall of the proximal pedicle. Dotted white line: medial pedicular line, Dotted white arrow: the direction of the Tuohy needle in the AP image. (D) Needle position of the conventional transforaminal approach and the paramedian interlaminar approach in the AP fluoroscopic image.
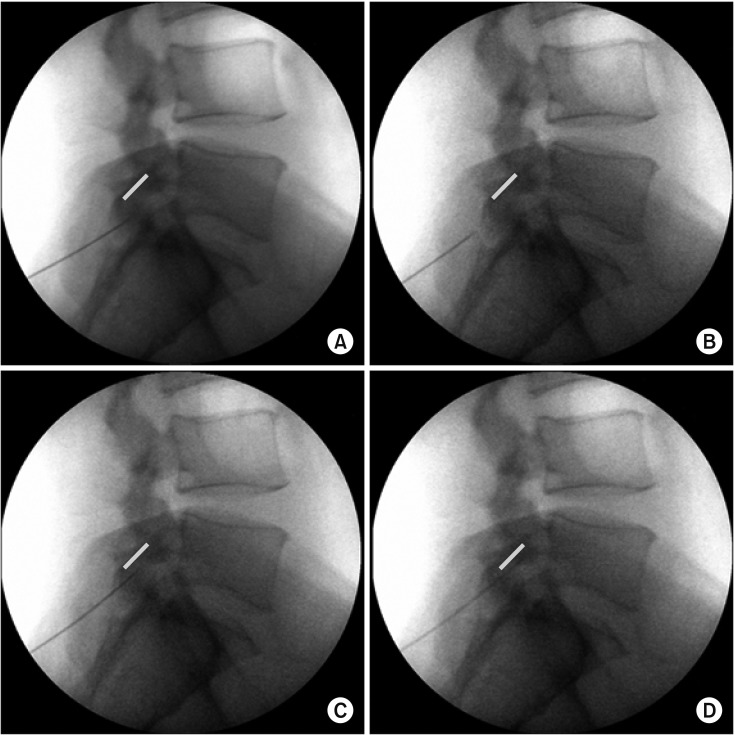
Fig. 2 Adjustment of the sagittal incidence angle of Tuohy needle. (A) Standard lateral image showing a Tuohy needle is stuck in the ligamentum flavum immediately after needle insertion. The Tuohy needle was pulled back (B) and its orientation was adjusted (C) to be inserted into the given neural foramen as close and parallel to the proximal lamina as possible. (D) Standard lateral image showing the Tuohy needle entering the dorsal epidural space through “loss of resistance technique.” Bold gray line: undersurface of L5 lamina.
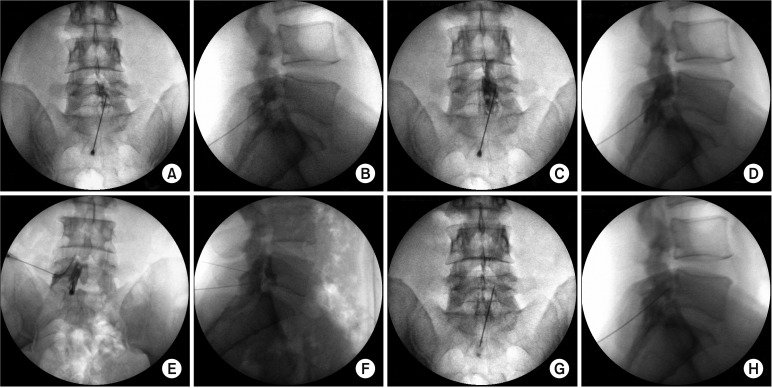
Fig. 3 Needle tip position and epidural contrast spread pattern. After placement of the Tuohy needle in the dorsal epidural space via the ligamentum flavum, 0.5 mL of contrast dye (Iobrix 300, Iohexol; Taejoon Pharm, Seoul, Korea) was injected to determine the contrast dispersal pattern on the anteroposterior (AP; A) and lateral (B) fluoroscopic images. The position of the end of the needle was on the outside of the L5 traversing nerve root in the coronal plane (A) and in the dorsal epidural space in the sagittal plane (B). Then, the needle was gently advanced until it touched the posterior aspect of the proximal vertebral body or the annulus fibrosus of the intervertebral disc. It was observed that the final needle tip position rose from the inferior pedicle line to the mid-height of the pedicle on the AP (C) and lateral (D) fluoroscopic images. It was also confirmed that the contrast medium spread out along the L5 exiting nerve root and S1 traversing nerve root (C), as well as into the ventral epidural space (D). However, in paramedian interlaminar epidurography, the needle tip was 10°–15° inward and located inside the lateral margin of dural sac (E), and dorsal epidural contrast spread (F) was observed. In conventional transforaminal epidurography, ventral epidural contrast spread (F) and periradicular infiltration (E) were observed along the L5 exiting nerve root. After drug injection, periradicular infiltration (G) through the L5 exiting and S1 traversing nerve roots was noted and contrast dye was observed to spread from the ventral epidural space (H) in the craniocaudal direction on the AP (G) and lateral (H) fluoroscopic images.

Fig. 4 Epidurography of a patient with subarticular disc extrusion and downward migration at L5–S1. The patient underwent a preganglionic epidural injection through the translateral recess approach. Plain anteroposterior (A) and lateral (B) radiographs showed lumbar spondylosis with discovertebral degeneration at L4–5. (C, D) T2-weighted axial magnetic resonance imaging showed previous left partial hemilaminectomy performed at the L4 vertebral lamina. (E, F) It was also observed that the left S1 nerve root was compromised by moderate left subarticular disc extrusion with downward migration. A preganglionic epidural injection was performed through the translateral recess approach. (G) In the anteroposterior fluoroscopic image, the contrast spread pattern for periradicular infiltration appeared as a hummingbird at the L5 exiting (beak, head and wings of a bird) and S1 traversing (abdomen and tail of a bird) nerve roots because of the filling defect caused by subarticular disc extrusion and downward migration. Gray curved line: periradicular infiltration pattern of the L5 exiting nerve root. White curved dotted line: periradicular infiltration pattern of the S1 traversing nerve root. White oval: filling defect of contrast dye for intervertebral disc herniation. (H) Photograph of a real hummingbird for comparison. (I) In the lateral fluoroscopic image, cranial and caudal contrast spread in the ventral epidural space was observed. Gray straight line: dorsal epidural contrast spread. Gray curved line: ventral epidural contrast spread. White dotted line: periradicular infiltration pattern of the L5 exiting nerve root.
Reference
-
1. Manchikanti L, Pampati V, Falco FJ, Hirsch JA. Growth of spinal interventional pain management techniques: analysis of utilization trends and Medicare expenditures 2000 to 2008. Spine (Phila Pa 1976). 2013; 38(2):157–168. PMID: 22781007.2. Bicket MC, Horowitz JM, Benzon HT, Cohen SP. Epidural injections in prevention of surgery for spinal pain: systematic review and meta-analysis of randomized controlled trials. Spine J. 2015; 15(2):348–362. PMID: 25463400.
Article3. Kabatas S, Cansever T, Yilmaz C, et al. Transforaminal epidural steroid injection via a preganglionic approach for lumbar spinal stenosis and lumbar discogenic pain with radiculopathy. Neurol India. 2010; 58(2):248–252. PMID: 20508344.
Article4. Kortelainen P, Puranen J, Koivisto E, Lahde S. Symptoms and signs of sciatica and their relation to the localization of the lumbar disc herniation. Spine (Phila Pa 1976). 1985; 10(1):88–92. PMID: 3983706.
Article5. Ebraheim NA, Miller RM, Xu R, Yeasting RA. The location of the intervertebral lumbar disc on the posterior aspect of the spine. Surg Neurol. 1997; 48(3):232–236. PMID: 9290709.
Article6. Shim DM, Choi YH, Yang JH, Oh SK, Kim CG, Park JH. Analysis and measurement of the lumbar spinal canal dimension using magnetic resonance imaging. J Korean Orthop Assoc. 2008; 43(5):588–594.
Article7. Xu R, Burgar A, Ebraheim NA, Yeasting RA. The quantitative anatomy of the laminas of the spine. Spine (Phila Pa 1976). 1999; 24(2):107–113. PMID: 9926378.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Persistent Hiccup after Epidural Steroid Injection: Case reports
- Epidural Steroid Injection
- Pneumocephalus after Epidural Steroid Injection: A case report
- Selective Epidural Steroid Injection in a Patient with Refractory Radicular Leg Pain: A case report
- Comparison of Transforaminal Epidural Steroid Injection and Lumbar/Caudal Epidural Steroid Injection for the Treatment of Lumbosacral Radiculopathy
